

As always, opinions in the following blog are mine, and not necessarily those of the Ontario Medical Association.
Recently, Canada Health Infoway, a non-profit organization funded by the federal government to develop digital health solutions, announced that their electronic prescription solution, PrescribeIT, was adopted by the Shoppers Drug Mart and Loblaw chain of pharmacies. This followed on the heels of PrescibeIT being accepted by the Rexall chain. PrescribeIT allows physicians to essentially send electronic prescriptions from their Electronic Medical Records (EMRs) to pharmacies directly, eliminating the need for paper prescriptions.
Reaction from many physician leaders was generally positive:
Other reports indicate how solutions like this have helped during the current COVID19 pandemic. In England for example, 85% of prescriptions are now electronic, thus helping with social distancing.
While I’m glad progress is (finally) being made, I’m forced to ask one question. Why did it take so bloody long?
As I’ve mentioned repeatedly to various health care bureaucrats over the years, my region (Georgian Bay) has had electronic prescriptions for ELEVEN YEARS now. We’ve regularly been emailing pharmacies and had them message us with either requests, or further information.
Our project additionally allows for pharmacists to become part of the health care team by allowing them limited access to a few important pieces of health information they need to do their job properly. For example, they are allowed access to the patients kidney function tests (knowing that many drugs are excreted by the kidney). In that way, I have gotten much advice about changing the dosage of medicine based on how someone’s kidneys are working.
Building on this project, our local area has also ensured that the our After Hours Clinic uses the local EMR, so if patients have to go there, the physician on call can easily access their charts. The local hospital allows us to house our server in their IT room (increases security because of all the firewalls). The advantage of this is that hospital physicians can access all the outpatient records if needed, and provide better care for patients. Even our local hospice has access to this so that patients can get the care they deserve during their last days.
We were even able, for a three years to have the nursing homes access and securely message our EMRs. The result was an over 50% reduction in admissions to hospital from the nursing homes. The cost of the project was $35,000 per year, but the government couldn’t find the right pocket of money to fund it (sigh – see here for how the bureaucracy works) and so the project died. If you need a cure for insomnia, my talk with more details of how the project worked is here (skip to 7:28):
This then is the real frustration that I, and many other physicians have with EMRs and other Health IT systems. Can you just imagine how much further we would be if all areas of the Province had what a few isolated regions (like mine) have?
For COVID19 for example, our Covid Assessment Centre is on our EMR which means that I get an automatic notification if someone goes for a test. And if that test is positive, it allows for quick notification of the family physician so we can begin the process of contact tracing. It also allows for easy transmission of information of people with febrile respiratory illnesses so that we can track important information like when the symptoms started and ended.
Dr. Irfan Dhalla wrote an exceptional piece in the Globe and Mail on preparing for the winter in times of COVID19. Unsurprisingly, he called for reducing “untraced spread” of COVID19 (50% of all cases have no known contact) and a large part of that solution is a technological one, namely the Canada COVID alert app (available at both the Apple App Store and the Google Play Store).
While he’s correct about that, the reality is that we have more illnesses that we have to deal with than just COVID19. We need to be able to manage cancer, other infectious disease, heart disease, diabetes, the frail elderly with multiple problems and much more. The better we manage those illnesses, the more we can keep those patients out of hospital, which is great anytime, but particularly when there is a risk of hospitals being overwhelmed by a pandemic.
Again, in our neck of the woods the Home Care case co-ordinators are on our system. I often get messages from them about how one of my patients is doing, and requests for information from them (so much easier than faxing). This allows me to remotely address concerns patients are having sooner, and for frail patients, getting treatments sooner can often prevent a rapid deterioration, which will of course, prevent a hospitalization.
So while I really am glad that many more physicians will have access to PrescibeIT, I reluctantly point out that in its current iteration it only does about 65% of what our solution does. I suppose that’s better than 0% which people had before, but it is a testament to the failure of a wide swath of health care bureaucrats over the years that this is the best we have.
Even our system is not perfect. I get miserable situations like some of my COVID19 results come in through OLIS (Ontario Lab Information System) and others through HRM (Hospital Report Manager) and yet others get faxed (!) to me. The auto-categorization in HRM is really a complete joke. I dictated a note on one of my hospital inpatients, and the system classified me as a combined General Surgeon, Anaesthetist and Paediatrician – and while I’m glad the system thought I was that smart, the reality is I now have to go through all this data and spend extra time categorizing it properly.
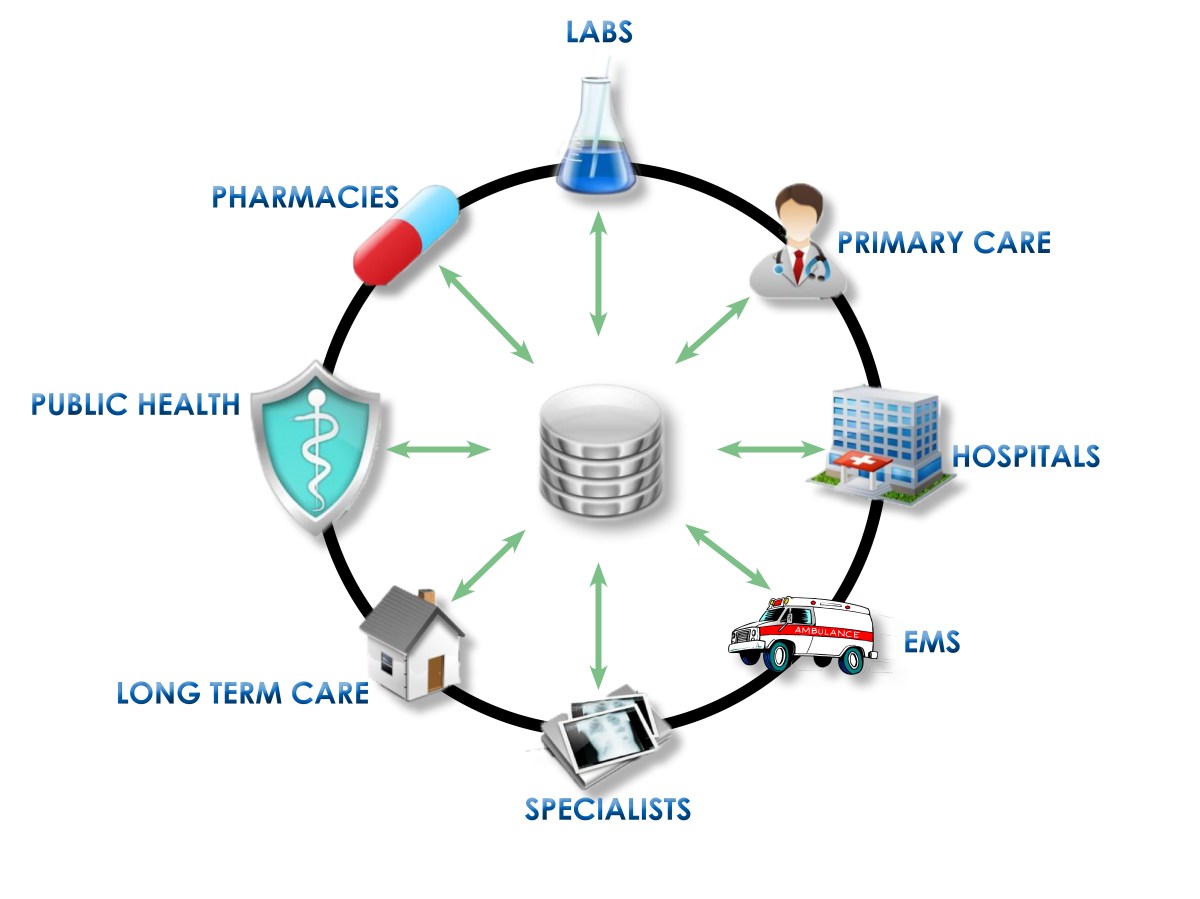
eHealth Ontario, Ontario MD, Health Quality Ontario, the Ministry of Health and its various digital health teams were all to work co-operatively to build a strong Health Information System. But the reality is that these individual systems do not share information in a way that benefits patients. The shared vision for health IT in the province (integrated health systems IT) still only exist in pockets around the province. There are lessons to be learned here and steps that should be taken. All of which would really be beneficial now as we head into a potential second wave of COVID19.
Which leads this old country doctor to wonder: If knowing that a potentially huge crisis is coming our way in health care, will no one step up with a vision to fix Health IT Systems and Integrate Health Care information once and for all? And if not now, WHEN?

2 thoughts on “Integrated Health Care: If Not Now, When?”