Wait, doc, what’s this all about? You’re asking people not to move to where you live?!?
Yes. Please don’t move to this area.
But you always tell others how wonderful an area this is!
This is indeed true. I love living here. I consider myself very blessed for having come here 34 (!) years ago. We are a few minutes’ drive away from the world’s longest freshwater beach, a few minutes’ drive away from ski hills. There’s golf, boating, too many outdoor activities to list. I enjoy the trails myself and often bicycle to my office during the warmer months. A true four seasons resort area.



Is the problem the people?
Not at all. The people here are kind, generous and extremely supportive. Plus there’s an old farmers mentality in a lot of them (that’s a good thing). I’m grateful they have allowed me into their lives. It’s an honour to help them.
Is the problem the growth in the area?
I’d be lying if I said I was completely happy with the increase in the population over the past ten years. The towns have gotten quite crowded, and the roads are busy. Bicycling on the roads is now classified as a survival sport. And yes, I have seen traffic jams, which is something I never thought I’d see. But no, that’s not it exactly.
Okay, doc, you’ve got me really confused. What exactly is the issue then?
It’s the healthcare system.
That makes no sense. You’ve often talked about how proud you are of the fact that you were the inaugural chair of the Georgian Bay Family Health Team, and how closely the doctors in the area worked together to form a really cohesive medical community.
This is true. The Georgian Bay Family Health Team, under the leadership of their Grand Poobah (inside joke), Maria LaRose, is, in my opinion, the best health team in the province. The doctors and allied health care staff all work well together. We formed the first community wide Electronic Records system in the Province. It’s still the only one in Ontario that is integrated with other health care partners. It’s the best medical community in the province.

Okay, so is it the hospital? Goodness knows you’ve had issues with administration in the past.
Actually, we’ve been very fortunate to have better administrators at the hospital the last couple of decades. The nursing staff and other allied healthcare professionals (physiotherapists, occupational therapists, pharmacists, respiratory therapists, and so on – apologies to those I missed) really are excellent and hardworking as a team. They really want to help patients. The problem, of course, is that they are overworked.

So then your issue is with the capacity of the local healthcare system?
Exactly. You see, currently, we have seven thousand people in our neck of the woods who don’t have a family doctor. If you move to the area, you will be number 7,001. Therefore, you will wind up going to our after hours clinic, or the hospital emergency department, which will increase the stress on those facilities.
This is, of course, not the fault of the individual physicians, nurses, allied health care workers. The blunt reality is the health care infrastructure is not there.
But I thought you guys were building a new hospital?
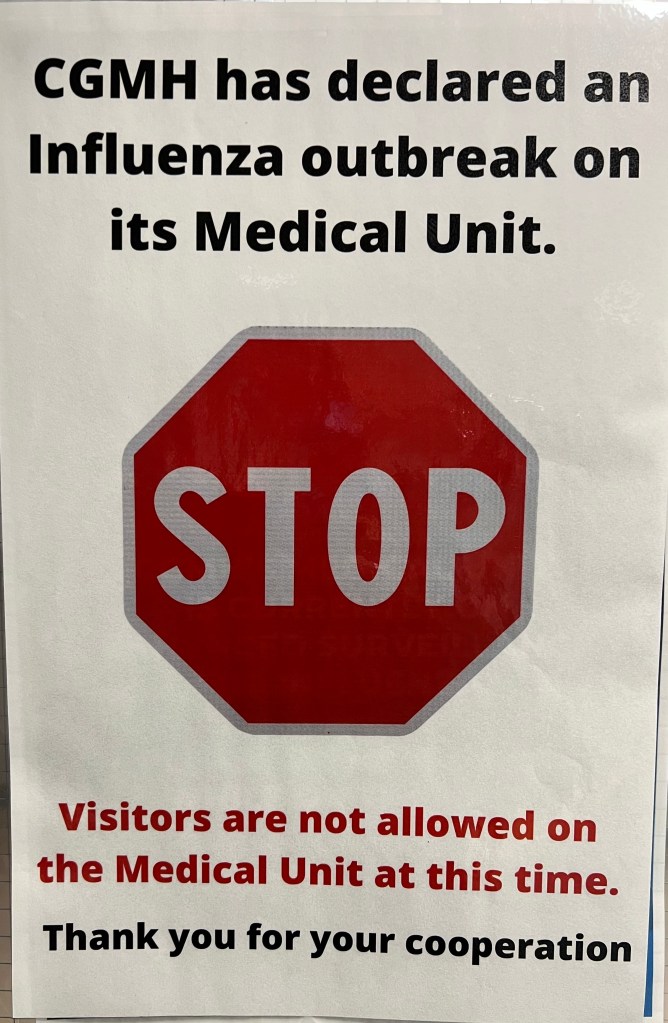
We are. BUT. We’ve known we’ve needed a new hospital since the early 2010’s, and despite many pleas, won’t start digging until 2029. We are hoping to complete in 2032. Various layers of inept government bureaucracy at the Ministry of Health have thrown many roadblocks in the construction process. As a result, our over burdened hospital puts patients in “unconventional places.“
You mean like hallway medicine?
Actually, I believe the term now is “chair care“because even the hallways are full.
Wonderful. Are the local townships not doing enough to recruit doctors?
It’s not really a township responsibility to look after the healthcare system. Now, there are some local efforts (with a bit of success) to get more family doctors in the area. However, that’s a slow process until the wider provincial problems are fixed.
You’re saying don’t come to the Georgian Triangle, but don’t these issues occur elsewhere?
Absolutely. I mentioned the Georgian Triangle just because it’s the area I know the best. Ontario has many beautiful areas for people to live in. Lots of different type of communities to suit all needs from small town, to large urban settings. But, if you currently live in an area where you already have a family doctor and you have a number of health issues, you really may want to reconsider moving until you can assure yourself of getting continuous, comprehensive, ongoing care in the community. Without a local family doctor, you will be getting itinerant care seeing different doctors at walk in clinics or Emergency departments, and that’s not good for your health.
So don’t move anywhere if you already have a family doctor?
Well look, people often have to move for many reasons. Work, family, retirement. I get it. BUT, I would encourage you, if at all possible, to scope out not just the amenities of the area you are thinking of, but also check the local health system out. That is something most people don’t do, they just expect health care to be there for them. That mentality needs to change.
And don’t move to the Georgian Triangle?
Yah, don’t move here. Our doctors (and hospital, and home care) are full.