This year’s Ontario Medical Association Annual General Meeting (OMA AGM) was more exciting than usual. There’s much to talk about. But to my mind, it appears that members have once again exerted a degree of control over their association. That is a good thing.
The meeting got off to a very inauspicious start when both Board Chair Cathy Faulds, and CEO Kim Moran blatantly misled (at best), or at worst, lied to the members. Both of them repeated how the OMA secured agreements with the government to provide significant funding increases for physicians. This is, of course, patently false. An independent third-party arbitrator imposed an award that the OMA and government have to abide by.


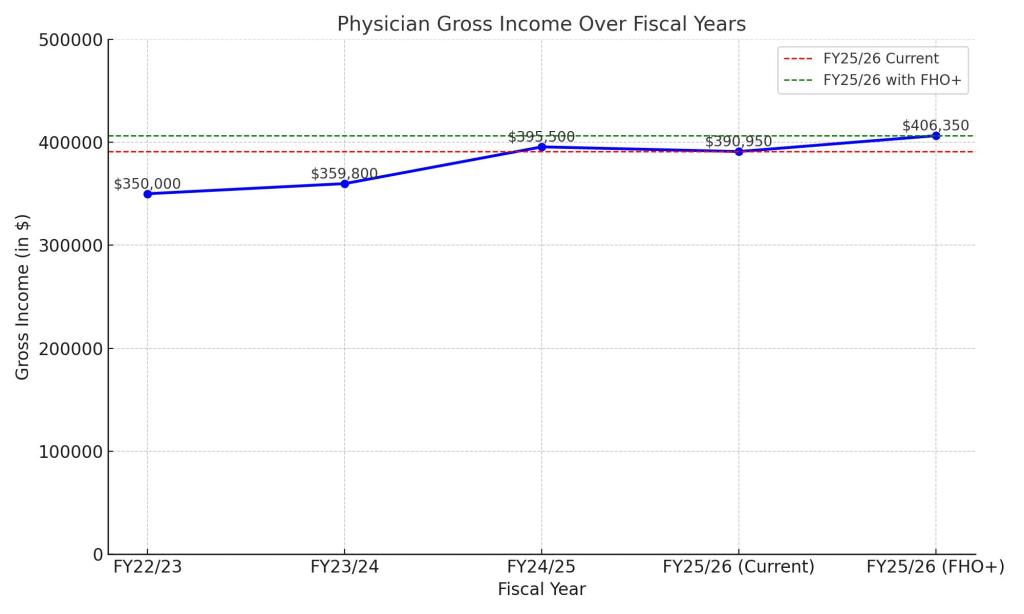
It is true that after the money was awarded, some aspects of the byzantine physician services contract were negotiated. Many others, including the much-hyped FHO+ program for family physician, were arbitrated. To suggest this represents an agreement with the government that was acceptable to everyone is insulting to members and outright false.
The highlights of the meeting were two speeches. First, by outgoing president, Doctor Zainab Abdurrahman (whose last name Dr. Faulds still couldn’t pronounce properly). I think she’s done a very good job as being spokesperson for the profession, no more so in her advocacy around trying to fix the outdated and incompetent OHIP billing system. Doctor Rebecca Hicks, the incoming President also gave what I thought was a truly inspiring speech. This bodes well for how she’s going to represent the profession in the future. And, it’s the first time the OMA has had two female presidents in a row – which is well overdue.


Unfortunately, the meeting went downhill from there. I will not blame the technology. I’ve attended many virtual meetings for many different organizations. The technology for the software is expanding much faster than the server resources are allowing, and so there are always going to be significant glitches. I also need to point out that the parliamentarian who was hired to run the meeting did an excellent job given all the limitations that he was facing. And I want to give a shout out to the frontline OMA staff who diligently tried to keep the technology moving.
Sadly, my criticism is going to be directed at many of the physicians who did their best to obstruct motions that were duly presented, met all the timelines, and followed the bylaws. Unfortunately, we physicians are sometimes done in by a small number of our colleagues who seem to think they know better than the rest of us, and can’t have us expressing our contrarian views. This was never more evident than last night.
Immediately after Dr. Conte’s first motion (to change the bylaws to remove non-physician Board Directors) came up, there was a motion to defer for one year. This was to let the Board create committees to “study the implications” of the motions. This is, of course, nonsense. One of the things the OMA did do fairly well is they put out a package on the implications of what would happen if these motions passed and if they failed. It was very thorough. It was available to every member who attended the meeting. The fact that some people chose not to read it is a reflection on them.
More suspiciously, the people who spoke out for the motions to defer were the usual suspects (double entendre intended for a couple of select friends of mine). The type that sign up for every committee and collect their stipends from members dues. Thankfully, the majority of attendees were going to have none of this, and deferral failed.
Unfortunately, this did not stop more shenanigans. There were all sorts of attempts to block this motion, questions about process, points of order – too many to remember really. But eventually, fifty-three percent of members at the meeting supported his first motion. However, the motion needed 67% to pass as it was a bylaw change.
This brings back shades of the motion of nonconfidence in the then Ontario Board Executive in 2017. That motion also required sixty-seven percent, but got fifty-five percent at council. The Executive eventually did the right thing and resigned. One hopes that the non-physician Board Directors, who by all descriptions are decent people with integrity, will see the writing on the wall and resign.
The fact that this motion actually had majority support sent supporters of the current leadership structure into a state of panic. The next motion, which would have removed the non-physician Board Directors, but at the end of their terms, only required fifty percent plus one to pass. This meant that this glorious structure that had been put together where the OMA chose candidates for board and not the members themselves, and the OMA could manipulate the elections to satisfy a select few was in danger. More motions to delay, more procedural gimmicks. More “we haven’t had time to study this.”
Eventually, as the meeting was running over time, the decision was made to defer the rest of these motions to another meeting that will occur within six weeks. This puts the OMA in the same kind of limbo that it was in after the board executive of 2017 was rejected but refused to resign. Not a good place for an organization to be.
More importantly, however, despite what I’m sure is being said about people like Drs. Conte, Hacker and yes myself, these events actually show the true power of the governance transformation. As the guy who was tasked with giving the speech to the then OMA Council to convince them to go down this path, let me state clearly that the driving force behind the transformation was always to give front line physicians power to control the organization if they felt it was not serving their interests. It has not been easy, or quick, and will drag on due to the shenanigans at the AGM, but members are exerting a level of control, and pressure over the OMA that they have every right to do. It may very well be painful for those in charge (they didn’t get their way) and it may very well require members to invest more time (yet another meeting), but it is a very good thing.
Ontario physicians deserve a strong and responsive OMA. This year’s AGM, as messy and complicated as it was, is a step in the right direction.
If you have any questions about the meeting, and what happens next, I encourage you to sign up for the OMA Webinar on May 13th at this link.