


NB: Recently, Julia Malott spoke out on X (formerly known as Twitter) about how terrified she was about Canada’s health care crisis. She wrote how her daughter had not eaten in 18 hours as she continued to wait for surgery for appendicitis. She expressed concern about the lack of the beds and wondered if her daughter would get surgery before the appendix ruptured.
My friend Dr. Soni, who has worked in an Emergency Department for over 20 years, had, as usual, a very thoughtful and well spoken X thread of her own. (Dr. Soni was NOT involved in the care of this young woman). I thank her for allowing me to reproduce her thoughts here.
The only way these stories (about long delays in Emergency rooms) will stop being the norm, is when patients start sharing their experience like this mother did. Only voters can make federal and provincial governments change because votes are the only currency that matter. Doctors and nurses have been raising alarm bells for years without success.
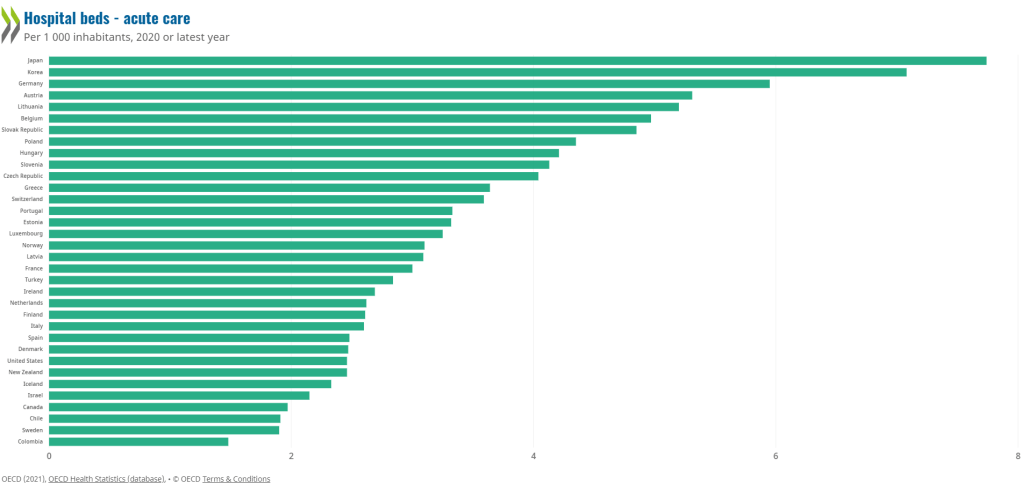
Canada has one of the lowest number of hospital beds of all the OECD countries, around 2.3/1000 people. In comparison countries like Japan, Korea and Germany are around 13/1000.
Why does this matter? Having low hospital bed numbers means that words like “flu surge“, and “winter surge” — which have been used for decades to explain away long wait times and hallway medicine, are actually not “surges.” Rather, they are the expected backlog in a system that lacks adequate beds and resources.
The population of Canada is increasing and aging. We are about to enter a silver tsunami where a large cohort of our population will be over the age of 65 and many over the age of 85. This will place unprecedented pressures on our health care system.
What happens when the hospital bed capacity is outstripped by the numbers of patients needing care? It means that the elderly patient who needs admission to a hospital bed to recover from a heart attack has no bed to go to and spends days “admitted” in the emergency department. Bureaucrats call these “unconventional spaces.” What they really are, are stretchers.

When the vast majority of the emergency department beds are being used to take care of hospital patients, that means that patients that are waiting in the emergency department waiting room, will wait for hours for care, much like this story is describing.
Media needs to scratch beyond the surface and hold government to account. Real solutions are going to require thinking beyond the four-year election cycle. What will our system look like in 20 years? How do you plan for that?
It’s going to require recognizing the backbone of our healthcare system is primary care. Family doctors are overwhelmed by administrative burden, trying to run their offices and taking care of large practises in the community without adequate resources.
Build community infrastructure with resources like palliative care so that people can remain in their homes comfortably in their last days; and sufficient homecare services so that patients can receive antibiotics and other intravenous treatments at home to ease the pressure on hospitals. These services are vastly underfunded and do not have enough staff to properly provide care for everyone that needs it in the community.
It’s going to require building more nursing homes, retirement homes, seniors services and dementia care programs, as our elderly population will be the largest it’s ever been in this country.
Incentivize and properly pay hospital nurses so that we can recruit and retain them to be able to run departments and programs properly. Currently, agency nurses make at least two times as much as a hospital nurse, and this has created instability in the workforce. Governments need to show that they value nurses and the important work that they do.
Creative solutions like interprovincial licensing of doctors and nurses and a National Pharmacare program will help. While the idea of recruiting from other countries sounds like an easy quick fix, it will not solve anything if those newly obtained doctors and nurses find themselves overworked and burning out soon after arriving to Canada. The system problems are going to impact them just as they have impacted those who are already working in the system. This type of strain is what contributes to moral distress and burn out.
The backlog in the emergency department is a reflection of multiple failing areas that create an overall system that is strained beyond capacity. With each passing year, Canada’s healthcare system has become more and more stretched, trying to provide more care to more people, with fewer resources. Throwing Band-Aids at it is like trying to mop up the floor under an overflowing sink instead of trying to figure out how to turn off the tap.
Stories like this one are happening every day in Ontario and all of Canada. Most patients and families are too busy dealing with the acute health problem to take the time to write to their MP/MPP or to go to the media. But when people take the time to bring these stories to light, a critical tipping point will eventually occur where they can no longer be ignored by government. Because votes matter.
No one who went into healthcare wants to work in a system that makes patients feel like this story illuminated. But we need more voices bringing their stories out in the open. It will improve the system for the people working in it, and for the people receiving care within it. And that is better for everyone.
