

Pharmacists do a great job as part of a health care team. In hospital and nursing homes, I get expert guidance on dosages of potentially dangerous medications. I am also fortunate to have community pharmacists on a secure electronic messaging platform to discuss issues around medication complications/interactions/dosages and so on for my patients.
But, will it improve health care to let them treat minor conditions?
I expressed my displeasure on Twitter about the recent move to allow pharmacists to treat certain minor ailments:
A few pharmacists were not amused. It was pointed out to me that Ontario is one of the last provinces to allow this, and that it has “worked well” in other provinces.
But what exactly is the definition of “working well”? Politicians love it, mostly because it allows them to say “see we are taking steps to make your life easier.” Patients love it because they can say, “Jee, I think I have a bladder infection, now I can just get the antibiotic when I want.” Of course patient satisfaction will be high.
Unfortunately, as I wrote about a few years ago in the Huffington Post, patient satisfaction does NOT correlate with good health care or outcomes. As counter intuitive as it may seem, higher patient satisfaction scores correlate with a 9% higher cost per patient AND a 12 percent higher hospital re admission rate. Patient satisfaction should not be used as a metric to determine any health care policy.
On Twitter, Nathan McCormick suggested that pharmacists have a lot to offer and linked to an article from New Brunswick on how it’s worked well there. Unfortunately (and I stand to be corrected) the article suggests the diagnosis of urinary tract infections was made without a urine culture, or even a urine dipstick test (which is less accurate but still something). So there’s no way to sort out how many people had a true bladder infection, or simply “felt” like they did, which happens. The article also puts a strong focus on patient satisfaction and convenience, which as mentioned above, is not the same as good health care.
Nardine Nakhla asked me to familiarize myself with an article she wrote about how Ontario developed the process. There’s a lot to like in what’s written there:
- A recognition of overprescription of antibiotics as a world wide problem
- a focus on ethical standards based behaviour by pharmacists
- A minimum amount of training for pharmacists before treatment minor ailments
- The requirement for pharmacists to contact the family doctor or nurse practitioner when treating a minor ailment
Once again this doesn’t really reflect true health care outcomes. It also references the aforementioned New Brunswick article and specifically stated there was high patient satisfaction there.
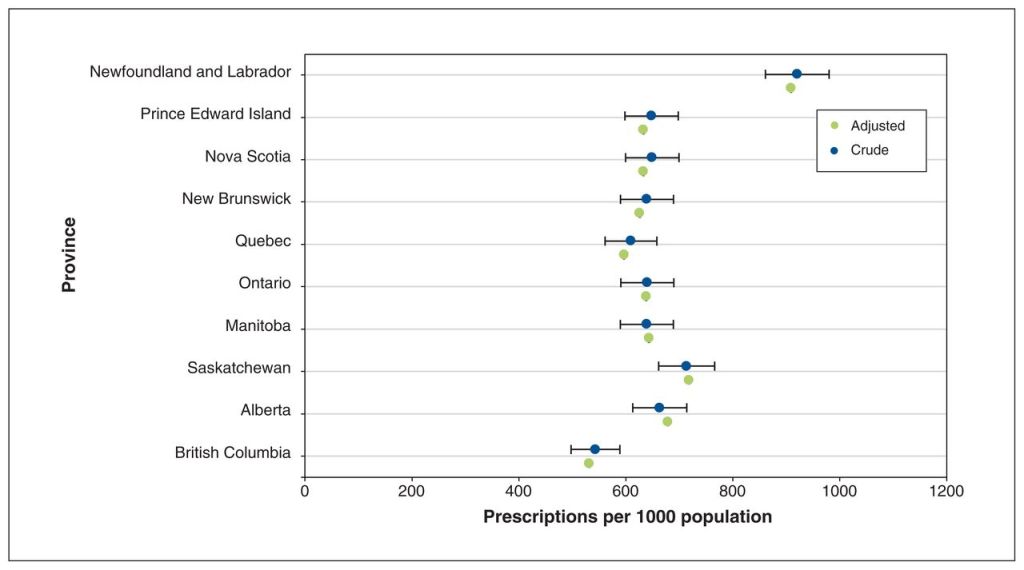
Let’s look at just one area of concern, antibiotic usage. Global overprescription of antibiotics is a world wide concern. It leads to increasing antibiotic resistance and the formation of new, drug resistant bacteria. A look at Canadian data shows that there is intra provincial variation in the number of antibiotic prescriptions. Newfoundland, where pharmacists have been treating minor ailments for years, has the highest rate of antibiotic prescriptions. British Columbia, where pharmacists are expecting an expansion of their scope this spring, had the lowest.
World wide , of the ten countries with the most antibiotic use, Cyprus, Romania, and Greece allow them to be purchased directly from pharmacies. (I stuck to EU countries with more modern health systems for examples).
Kristen Watt wrote a piece in the medical post criticizing physicians for complaining about these new powers and asked me on Twitter to provide evidence from other locations. She stated that Ontario was “15 years behind the trailblazing Alberta”. And yet the data in the CMAJ article above shows that Alberta has a higher rate of antibiotic prescriptions per capita.
One area I do agree with her is when she wrote:
“the government roll-out video, shot in a noticeable big box pharmacy, didn’t help us”
That big box is Shoppers Drug Mart, and their CEO Jeff Leger is seen promoting this change on the video. Shoppers Drug Mart recently invested $75 million in Maple, a virtual care company. Maple’s home page still shows the following:

Gee, if you think you have a sore throat, you can just call a company (that Shoppers invested in), and get an antibiotic without a throat swab (who cares if it’s really strep) and lo and behold, there just happens to be Shoppers nearby that will deliver it to you. Yes, I know patients can request the pharmacy of their choice, but….
Look – there are other aspects of this process that need review. Accurate diagnosis of a rash for example (several of the new pharmacist powers are for skin ailments). Or communication with the patients family physician about the treatments given. Probably more.
I WANT pharmacists to help. I really truly am grateful that so many are willing to step up in a time where our health care system is collapsing faster every day. But I want pharmacists to help in ways that support good health care outcomes.
Might I offer three suggestions for how pharmacists can do that:
- As a group, they can petition Shoppers Drug Mart to put pressure on Maple to change the example on their website. It’s great marketing (focusing on convenience) but terrible health care.
- Get involved with Choosing Wisely, Canada’s leading group looking at all ways to pick the right health care treatments. There doesn’t appear to be a pharmacist in looking at their leaders. I think pharmacists could provide extremely valuable information on not just anti-biotic stewardship, but also overall medication management (eg. reducing pill burden in the elderly)
- Strongly lobby the government for a unified integrated electronic health system that will allow them secure communication with physicians and access to limited health care data (eg creatinine clearance). We’ve got this in my neck of the woods, and it’s a huge benefit to physicians, pharmacists and most importantly patients.
In order to save what’s left of our health care system (if that’s even possible now) we need to focus on health care outcomes, and ensuring proper an appropriate care. Doing the three things I listed above would be a big help in that direction.

I am a pharmacist and agree with you totally. Health care fragmentation is not a good thing. The rank and file retail pharmacist does not want this added responsibility when we are drowning in our regular tasks. Owners of pharmacists of course like this because they profit from it. The employee does not contrary to what people think. We are hourly employees just like the gas pump attendant and that is that. We are not even subject to meal breaks under employment law. I see my role as making sure the right medication gets to the right person in the right dose. I am happy to help and physicians and nurse practitioners with drug related questions. And of course navigating the patient’s insurance issues. I do not feel that diagnosing illness is in my purview. Of course patients/customers are happy when they get ‘something’ – it’s the expectation and ultimate outcome of any interaction. Trust me the rank and file front line grunt retail pharmacist is not asking for this.
LikeLike