I’ve been involved in medical politics for some time and in health care for much longer. I’ve seen a lot of foolish things. And yet, I confess, I’m still dumbfounded when some really smart people come up with a really stupid ideas. I guess I’m just a slow learner.
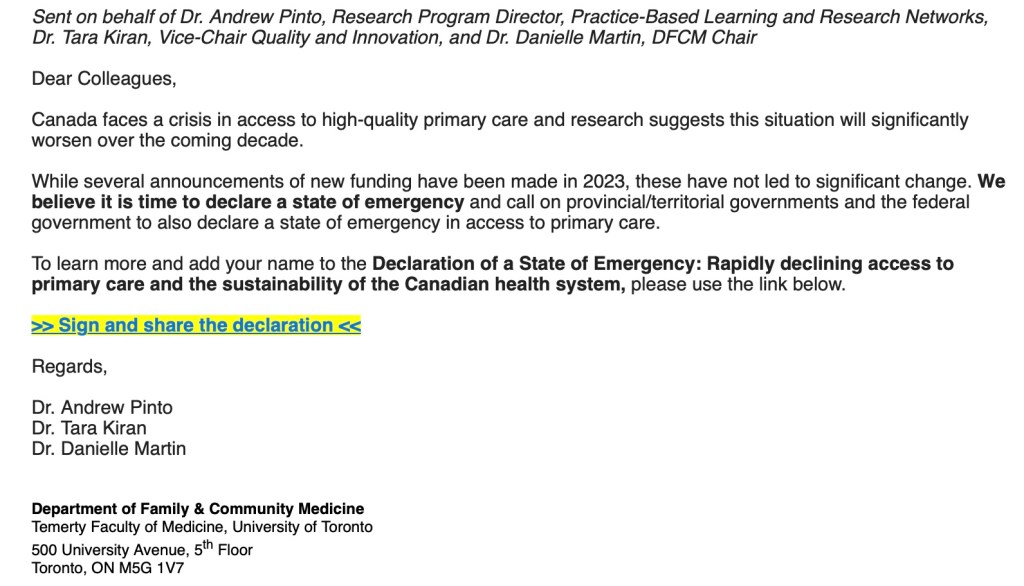
The most recent of these ideas comes from the Department of Family and Community Medicine (DFCM) at Temerty Faculty of Medicine. (Temerty is the name for the University of Toronto Medical School – and no, I have no idea when or why they changed their name to Temerty). In an attempt to address the crisis in Family Medicine, Drs. Pinto/Kiran and Martin would like the governments to declare a state of emergency in access to primary care.
Do I understand wanting to draw more attention to the crisis in Family Medicine? Of course I do. Family Doctors are planning to leave the field in droves. Compensation for family medicine has failed to keep up with inflation much less given them a raise. The admin burden makes one feel like Sisyphus (In Greek mythology Sisyphus was dammed by the gods to roll a boulder to the top of a hill only to have it roll suddenly back down to the bottom when it got close to the top and thus be forced to roll it up again. A more apt description of the family medicine paperwork burden I have never seen).
Heck across the country our whole health care system is in crisis, not just family medicine. Patients are not getting timely specialist care (some even choosing euthanasia as a result) as well as family practice care, resulting in worsening health care outcomes for all Canadians. We should be screaming about this.
But I honestly don’t think Drs. Pinto/Kiran/Martin (who combined have more letters after their name than the entire alphabet) could possibly have thought this recommendation through. Frankly, I’m genuinely left wondering if they even know what the government declaring “a state of emergency” means. The only way to enact this, is to invoke the Canada Emergency Act.
This Act clearly lays out what governments can do to solve a crisis in any particular area. And it’s not pretty. It includes:
- giving the government the “ability to make orders or regulations that are believed, on reasonable grounds, to be necessary…”
- Directing specified persons to render essential services…
- Regulating the use of specified property, including goods…
- The imposition of fines or imprisonment for contravening on any of the measures declared..
In short, having the government declare a state of emergency gives them a whole lotta power to do a whole lotta things. I guarantee you not all of those things will be smart.
No one in their right minds is going to argue with the issues identified in the letter three doctors wrote about:

The crisis in family medicine is real. There has been a lack of investment in primary care. This will get worse. This will cost the health system more money in the future if we fail to fix the problem. And yes, thank goodness somebody other than a cranky cynical old country doctor wants a significant overhaul and feels that “modest changes are not enough”.
But – to tell the government to enact a state of emergency, giving the same bureaucrats who have completely screwed up the health care system for the past thirty years almost unfettered power is not the solution. Let’s look at some of the goals of these three doctors:

If there is a state of emergency – do you know how these pointed headed bureaucrats will take “decisive action” to “ensure every person in their jurisdiction has equitable access”? You think they will licence more physicians? You think they will allow Ontario Health Teams (OHTs) to have strong physician leadership (which is the ONLY thing that has been proven to work in accountable care type organizations like these OHTs)?
I got news for you. The pointy headed bureaucrats will simply mandate zones, unilaterally determine how many patients a doctor must roster, and will make decisions in the interests of “urgency” given the new powers they just got from a state of emergency to show they are doing something.
Say for example the recent situation when Royal Victoria Hospital had to close down their obstetrics service. Hell that Gandhi fellow delivered babies 20 years ago, he probably hasn’t forgotten what to do – send him there to cover so it doesn’t close, he’s only 45 minutes away. Or a hospital about close their ER again – force a local doc who hasn’t worked in ER for 15 years to do so. 7,000 patients without a doctor in a certain town? Have each family doctor take a couple hundred more – even though those docs are already working night and day. (Trust me – these ideas will not sound outlandish to bureaucrats.)
Drs. Pinto/Kiran/Martin know that to make inroads into solving the primary care crisis you need to do three things:
- increase the payment to family physicians to reflect the work they do. Decades of sub inflationary wage increases (cuts by another name) have made it untenable to run a family physicians office. Pay family docs more and don’t be afraid to say so.
- The OHTs actually have potential for improving health care, but they need strong family physician leadership – not any other health care professional (and certainly not bureaucrats) – family physicians need to lead this. (The OMA has plenty of evidence on this and has shared with the government and will share with you).
- Interchangeable IT technology that allows easy access to patient data and thus minimizes the admin burden.
The only reason I can think of for doing this is some sort of political stunt to embarrass the politicians. Heck I agree politicians should be embarrassed for how badly they’ve messed things up. But to do it in a way that gives them more power (not less) instead of demanding a true collaboration with family physicians doesn’t strike me as a very smart move at all.