Dear Premier Ford,
Just me again, your erstwhile, somewhat (but not completely) humble old country doctor. Like last time, I would point out that I am really not your harshest critic. I want to recognize that you have done much for health care infrastructure over the past few years.
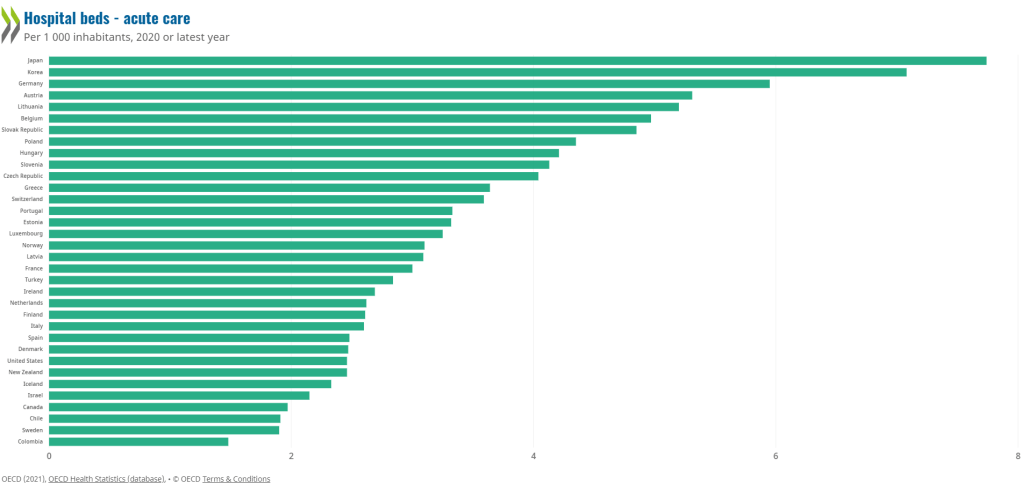
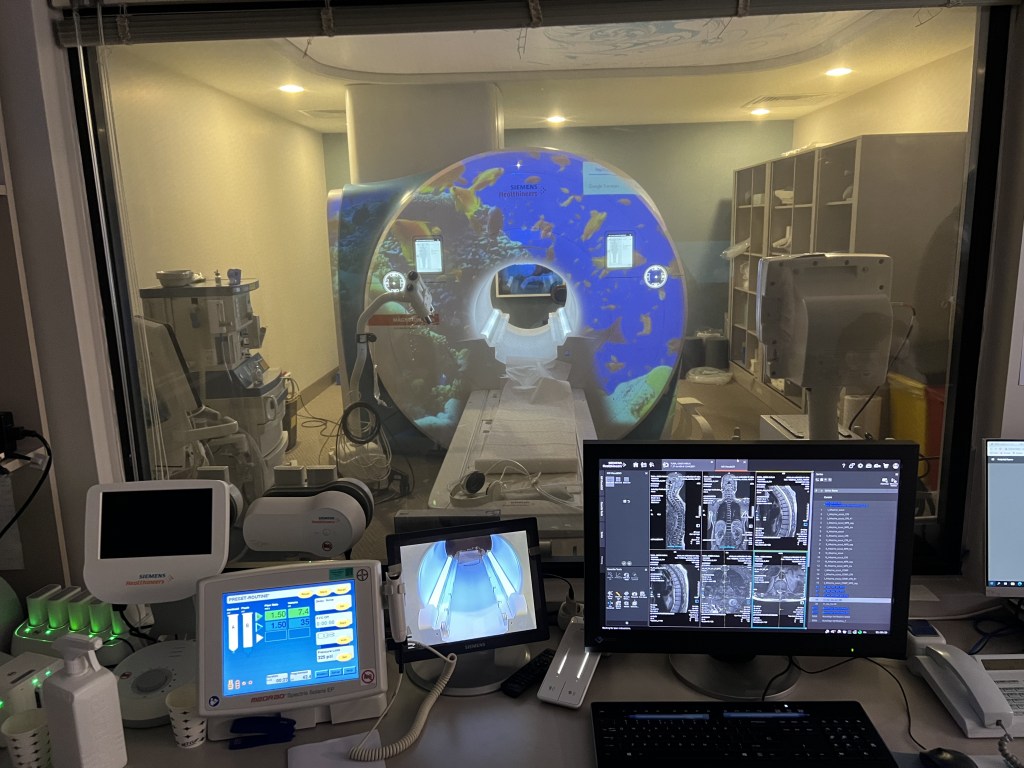
For reasons that I cannot fully explain, the previous Liberal regime simply stopped building the necessary infrastructure to help Ontarians. Whether it was new (badly needed) nursing homes, new hospitals, or new teams, the Liberals basically did, well, nothing in terms of infrastructure. To your credit, you’ve reversed that trend and are building facilities we in Ontario need. (As an aside, you seem to like building things a lot!)

But all of that building will not mean much in two years (when the next election is – nudge, nudge, wink, wink) if, as projected, over 25% of Ontarians don’t have a family doctor. Yes, you can correctly point out that the decline in family medicine was caused by the Liberals (it truly was – Eric Hoskins was by far the worst Health Minister I personally have seen in my time in health care). You can point out that the Liberals slashed the capitation model favoured by most family docs that started the downward trend. You can also point out that their favoured Deputy Health Minister Bob Bell thought family medicine was so easy he could return to it after over thirty years away:

He even tried to mansplain one of the true leaders of family medicine on how the system should work.
It’s true Bell and Hoskins were completely wrong. That will NOT matter because by 2026, the general public will say – “well you’ve had 8 years to fix this – you haven’t done enough”. That’s just how politics is, and I think deep down you know that.
You can, truthfully, also say that you are listening to organizations like the Ontario College of Family Physicians or the Ontario Medical Association (OMA) and who continue to go on about how team based care is the future of family medicine and how it can help solve the problem. You may not know this but I was the founding Chair of the Georgian Bay Family Health Team . I happen to believe in physician led team based care.
But here’s the thing. It will take a minimum of five years (if we’re lucky) to build out all those teams. That’s assuming the bureaucrats from the Ministry GET OUT OF THE WAY and let front line family physicians be in charge of the teams. But we are losing family doctors by the week. The people of Ontario can’t wait five years.
There is one thing that can be done now however, to stem the tide, and stabilize the system. You need to give comprehensive care family physicians an immediate, and significant raise. How significant? You will need to give an immediate 35% increase to comprehensive care family docs along with annual normative increases for the next four years. If you think that’s outrageous – I invite you to look at Manitoba’s contract or Saskatchewan’s or British Columbia’s. The competition for comprehensive care family doctors has increased significantly, and Ontario is falling behind.
I can pretty well guess what your “advisors” are telling you. They will say you are in arbitration with the OMA, just promise to abide by the result. Honestly, I do believe you will abide by the result, both this year and next.
But…
Arbitration will take months this year, and months if not a year next year. Frankly, I doubt that the OMA, despite their strong words, will advocate for an increase of the amount necessary for comprehensive family medicine (hopefully I’m wrong).
I have absolutely no doubt that the Arbitrator, William Kaplan, will give a raise to family docs, especially after the recent award to nurses. But if the raise isn’t enough, you going out to the general public in two years and saying “we honoured the arbitrators rulings” – will make zero difference to the close to five million people who won’t have a family doctor. They will still blame you for not having been pro active.

Listen, I’m on the conservative side of the political spectrum. I’ve always voted for the Conservatives in every provincial election since I was eligible to vote. I live in Simcoe – Grey which is one of, if not the most strongly conservative ridings in Ontario. Heck, in the early 1990s we were the ONLY riding east of Manitoba to vote for a Reform Party MP.
I’m telling you that most of the voices on the ground are really upset about the lack of family doctors. We have about 7,000 patients without a family doctor in our area last I heard. It’s true that when asked who they will vote for in polls, they, like most recent polls, say they’ll vote conservative. However, they always add “I guess, there’s nobody else out there”. That softness in your vote is a problem, and that softness doesn’t show up in the poll numbers.
Listen, I want you to win the next election. I personally think the NDP would be a complete disaster. I have no faith the Liberals, who showed just how much they hate doctors, have changed their tune. But in order to do that, you’re going to need to bite the bullet, and stem the haemorrhage of family docs.
Go to tell your negotiations team to offer up a deal that strengthens family medicine. Mask the increase with things like retention bonuses (like Manitoba) and matching RRSP payments (like BC) and other methods (paid admin time, paid supervision of team members and pensions would be nice). But get it done ASAP.
Otherwise, I genuinely think you will be in more trouble than you might be led to believe by your handlers in 2026.
Your sincerely,
An old country doctor.