Another in a weekly series of brief snippets of health care stories that bemused, intrigued and otherwise beguiled me over the past week along with my random thoughts on the matter.
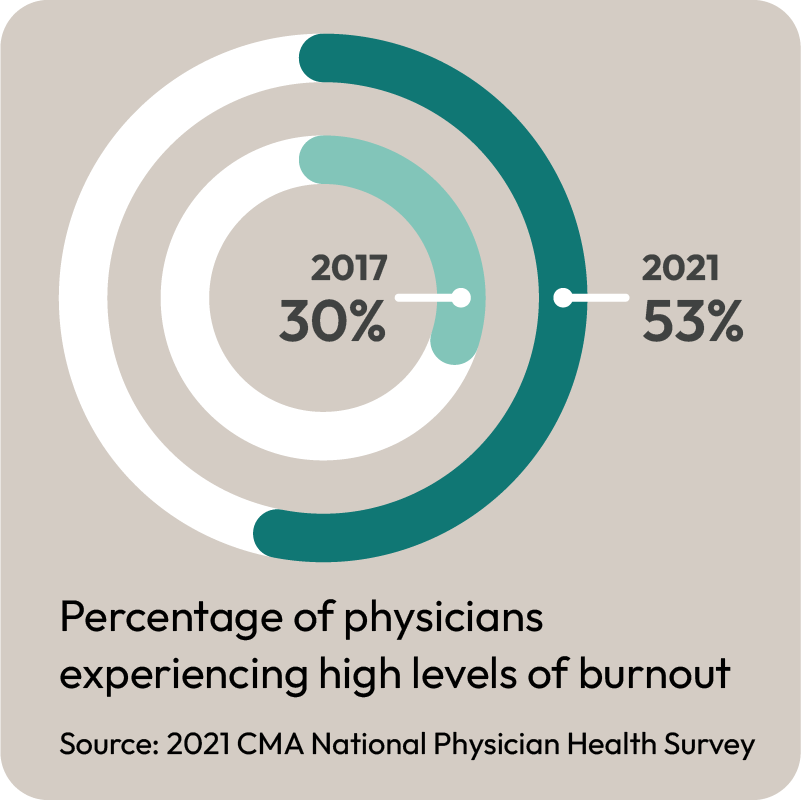
Item: Dr. Sarah Giles writes in the CBC about how she was forced to cut her hours because of the burnout.
My thoughts: Kudos to Dr. Giles for talking so openly about this. Alarmingly few of my colleagues are willing to talk about burnout and how the system is affecting them. Instead they suffer in private, and that’s not healthy for them OR the patients they serve. It’s an important story that needs to be told over and over again.
Item: “Involuntary medical treatment” for people with addiction issues seems to be all the rage. A great article in the “Conversation” shows that this won’t solve anything, and in fact will make things worse.
My thoughts: I really can’t believe we are even discussing this. It has been well known for…..well forever, that people will not get better unless they want to seek help. We have to focus on making seeking help easier, not forcing them.
Item: The always excellent Dr. Katelyn Jetelina, who most of my colleagues know as a superb voice of reason and information during the height of the Covid pandemic, writes about her feelings now that RFK junior has been nominated to lead Health and Human Services in the United States.
My thoughts: My heart goes out to her and all the hard work staff who have tried keep us all safe during the pandemic. They deserve better.

Item: TV Ontario had a segment suggesting that foreign trained physicians could help tackle Ontario’s physician shortage.
My thoughts: I’ll shout it out again, we already have enough family doctors in Ontario who are already licensed to practice medicine in this province and are familiar with the Ontario Health Care system. The number is approximately 6,000 or so (see the graphs in the linked blog for details). Can we just not make it easier to practice family medicine instead??? If we can get even 1/3 of those doctors already in Ontario to start a practice, we would end this crisis.
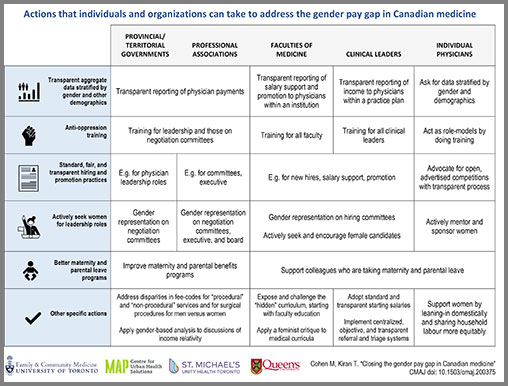
Item: Great article on the physician gender wage gap in Health Debate. Clearly shows that the gap is real and needs to be corrected.
My thoughts: One of the best accomplishments of the OMA Board when I was on it was to publish the gender pay gap report. It was arguably too late, but I believe we were the first PTMA to discuss this and to use that as a basis for future negotiations work. While I’ve had some issues with how negotiations have been handled since, I am quite comfortable in saying that positions of the OMA in negotiations would take this into account and that there is likely to be funds demanded to narrow this gap. The blame for the fact that there has been no progress on this lies mostly at the feet of the Ministry of Health. We don’t have an agreement yet on how to divide the arbitration award – and that means the Ministry is not responding to OMA proposals that would close this gap. Shame on them.
Item(s): Alberta announced that it hiring a large number of nurse practitioners to become “primary care providers” to patients who don’t have a family doctor.
My thoughts: The National Health System (NHS) in Britain is under fire for the fact that it too tried to replace the work done by fully trained physicians, with staff who were likely well intentioned, but had less qualifications. It turns out there is significant risk to this, and likely a markedly increase cost in providing health care. The article “My wife died because the NHS used cheap labour” should be, in my opinion, required reading for any politician/health care bureaucrat who thinks they can provide better care by using less trained people.
That’s all for this week. Back next week (probably) with more.