NB: My thanks to Dr. Tristan Brownrigg for guest blogging for me today. By his own admission, he never planned to be political, or seek out the limelight. But the situation in Ontario is such that he felt his perspective should be heard. I have a great deal of respect for people like Dr. Brownrigg, who are willing to step out of their comfort zone when necessary, and I commend him for doing so.
Dr. Tristan Brownrigg: I am a family physician, outdoorsman, and rural generalist currently working a mix of clinic, ER and inpatient care in the East Kootenays of British Columbia. I graduated from the University of Toronto Medical School, and did my Residency at Queen’s University (Kawartha site).
I completed family medicine residency in Ontario in 2022 and worked there for 6 months. Prior to this I completed medical school in Ontario, completed my undergraduate in Ontario, and had called Ontario home. Over the years I had watched my goal of working as a comprehensive rural family physician slowly become unsustainable amidst a collapsing system, decades of funding stagnation and poor planning, with a patchwork of good people on the ground trying to do their best in a system that doesn’t seem to value their input. Day after day the insidious march of the family medicine crisis grew closer to the forefront of peoples’ lives and garnered wider media attention, while the government either denied its existence or made no substantive changes that would realistically address it. This has not been the time for band-aids, let alone denial.
Last year I moved to rural British Columbia to try something different for a year, cautiously optimistic about the significant changes to family practice on the back of the LFP model implementation in early 2023. The Longitudinal Family Physician (LFP) model significantly changed how family physicians billed and were compensated in BC, including the ability to bill for the many hours family physicians typically spend on previously unpaid administrative tasks.
My experience has been night and day. For the first time in my medical career I have felt hopeful about the future of family medicine and find my day to day life to be sustainable. These changes have been received positively amongst all other family physicians I have discussed it with. It is not perfect and there are still kinks to be ironed out, but I at least believe my provincial medical association and government are trying to improve things for family physicians. I am not left questioning if government actions are purely incompetent or malicious with the intent to drive privatization.
I had retained my Ontario medical license until now, awaiting the May 2024 renewal deadline unsure if I would return home after a year of trying on a different life out west. Reading the recent government positions and negotiation briefs has been the final nail in the coffin for me. The disdain the Ontario government shows towards the hardworking family physicians who hold up the medical system is nothing short of repugnant. After more than a decade of training and education here, I will now be relinquishing my license to practice medicine in Ontario and stay in British Columbia.
The minister of health thinks recruitment and retention is “not a major concern.” That’s the problem; it should be. If I am not a prime example of this, I don’t know what is.
I wish all of my colleagues still in Ontario who do not have the luxury to vote with their feet the best of luck. If not this government, then I hope the next one learns to value your work and dedication.
My thanks to Greg Brady and 640 am News Toronto for interviewing me today (May 9, 2024) about comments from the Health Ministry that recruitment and retention of physicians is not a concern for Ontario. Posting a link to the podcast of that interview here, as some forms of social media will not allow the actual link to be posted.
On May 6, as part of a needlessly protracted negotiations process, the Ontario Medical Association (OMA) and the Ministry of Health (MOH) began public arbitration hearings to determine a compensation package for physicians for the fiscal year April 1, 2024 to March 31, 2025. Yes, arbitration has begun AFTER the last contract expired, and physicians will need to be given retroactive pay.
This is happening as part of the Binding Arbitration Framework (BAF) between the OMA and the MOH. When the two sides can’t agree on a compensation package after a defined period of time and negotiations, arbitration is invoked. The expectation is that arbitrator William Kaplan will issue an award sometime in August. It’s possible the two sides may reach an agreement before then as negotiations are allowed to continue during arbitration. It’s not unheard of that arbitration can sometimes pressure two sides to get a deal done before a decision is rendered.
William Kaplan, of Kaplan Arbitration Services
One common misconception I hear from my colleagues is that Mr. Kaplan will have to pick one side or another. That’s not the case. The BAF we have is for something called Binding Interest Arbitration. Mr. Kaplan will likely award something in between.
Public arbitration, is just that. It means that the arbitration briefs submitted by the two sides are public, and the arbitration hearings are public. Which means that physicians across Ontario know exactly what the government thinks they are worth. And that knowledge will demoralize an already disheartened profession.
Having gone through this process as an OMA Board member in the past, let me acknowledge a few things right off the bat.
Arbitration is still a lot better than the alternative, which would be unilateral government action. We’ve been down that road before during the Hoskins/Bell years and that was just plain awful for not just physicians, but patients as well.
As part of the arbitration process, the government purposefully put a “lowball offer” forward. Basically they know the arbitrator will likely award more than they offer so of course they try to present a lower version than they normally would expect.
In that vein, I would have expected the OMA to present a higher request. All physicians deserve a raise, and their proposal does address that. But the ask frankly just catches up (barely) for the last few years so calling their brief a “strong” demand is inaccurate.
Our negotiations counsel, Messrs Goldblatt and Barrett, frequently told me that it is much better to have a negotiated settlement that both sides agree to, than one that was forced on them by an impartial third party. More chance of the two sides willingly implementing the many nuances in an agreement as complex as the physicians one.
Howard Goldblatt, Negotiations co-Counsel for the OMASteven Barrett, Negotiatons co-Counsel for the OMA
However there is one thing that hasn’t been considered. Arbitration frequently leaves bad feelings amongst the two parties. In the sports world for example, one has to look no further than Toronto Maple Leafs goalie Ilya Samsonov. He took the team to arbitration last summer. The team clearly said some negative things about him to justify their offer to him. While the team has not exactly been forthright about what exactly was wrong with him mentally, there can be no doubt that he had a terrible first half of the hockey season. It was so bad he eventually got demoted (on paper) to the farm team – and his play was so bad no other team in the NHL wanted him (ouch).
Toronto Maple Leafs goaltender Ilya Samsonov
This is why sports teams try to avoid arbitration – they know that the process can be ugly, and can adversely affect the performance of their top athletes who have to listen to negative things said about them. For teams to succeed, the top athletes have to play their best.
Looking at the situation in Ontario, it’s frankly hard, as a physician, to feel anything but insulted and disrespected by how the MOH negotiations team has acted. It’s bad enough that they appear to have, for the most part, stalled the negotiations to the point where arbitration is needed. Contrast this with Manitoba, Saskatchewan and British Columbia, where the governments realized that they needed to retain their physicians due to the current crisis in health care, and made widely applauded agreements with their doctors. But Ontario’s arbitration position is so pathetically inadequate (even when considering they are low balling for arbitration) that one really has to wonder if they want to have good relationships with their doctors going forward.
From 2020 to 2023 – inflation has gone up by 14.8% (with another 2.9% for this year so far). Nurses were given an additional 6.75% (on top of their previous agreements) due to the unconstitutionality of Bill 124. And yet the MOH thinks physicians should only get three percent?? With no recognition of administrative burden? And the MOH claims there are no retention/recruitment issues?? Have they talked to the over 2 million people without a family doctor??
Does their negotiations team truly understand the harm they are doing by putting forward such an insulting and offensive proposal??
Here’s the thing, after a contract is agreed to or arbitrated, physicians and government will need to work together for the benefit of the people of Ontario. Yet how does any reasonable person expect physicians to work with a government team that on the one hand says that “physicians are valued and respected” but then, at the first chance they get, demean them with such a pathetic position.
Remember, many of the bureaucrats who provide supporting information to the MOH’s negotiations team have other roles. They’ll show up on other bilateral committees between physicians and the MOH. And after you denigrate people so badly with such an abhorrent brief, will there really be any trust between the two sides (and yes, they are now sides – this opening position makes it clear we are not on the same “team”).
Just like the Leafs needed Samsonov to, you know, make a few saves earlier in the season, the government needs physicians at their peak to deal with and give their best advice on the current mess that is health care. And while physicians, as is their nature, will genuinely try their hardest to do so – the blunt reality is that Samsonov tried his best to make more saves as well. But when your head is not in the right space……..
At this point there really is only one solution. The MOH negotiations team needs to formally apologize to all physicians for their incredibly repulsive offer. Then they need to look at BC, Manitoba and Saskatchewan, and put together a fair and competitive agreement so that more physicians don’t look elsewhere. This can be done tomorrow.
Recently, physicians leaders have been in the media promoting the right to primary care. I generally refer to this as a “Health care for All” policy, as it is reflective of one of the tenets of former Health Minister (and current Dean of Queens Medical School) Dr Jane Philpott’s new book. Dr. Tara Kiran has also promoted the same through her “Our Care” project. These proposals seek to guarantee a family physician for everyone in a certain geographic area, just like children in an area are guaranteed a school.
Dr. Jane PhilpottDr. Tara Kiran
While these policies sound nice (for reasons I’ll go over later) – they are doomed to failure. To understand why, let’s look at just two other situations – The Barer Stoddart Report and the move toward safe injection sites and decriminalization of illicit drugs. I appreciate my three loyal readers (I actually gained one!) might be wondering what this has to do with primary care. Bear with me, it hopefully will make sense later.
The Barer-Stoddart report is infamous in Ontario medical politics. It’s the report that is widely viewed as suggesting Ontario had too many (!) doctors in 1990s and led to the reduction of the number of medical school positions. However, what is not commonly appreciated is that was the last recommendation in the report. The first recommendations were to support the current supply of physicians by adding a large number of allied health professionals and making many health systems modifications. If and only if all those recommendations were carried out, then medical school enrolments could be cut. The bureaucrats and politicians looked at that, went through the report, decided that all the other recommendations were too expensive or complicated, and just cut med school enrolment. “The report told us to.”
Similarly, when it comes to drug decriminalization, the idea is best implemented in Portugal. The top line read is “addiction rates fall 40%” after Portugal introduced this policy. BUT a deep dive shows that before decriminalizing drugs, Portugal made a number of legislative changes, ensured that the court systems were educated, ensured that addiction therapy and counselling was available for addicts, and then implemented the decriminalization policy.
In Canada, our bureaucrats looked at Portugal, and figured all the rest of the changes were too complicated. But hey, maybe just decriminalizing will be enough without the other stuff! The result is a disaster when it comes to safe injection sites and an obviously failed policy.
So let’s look at the right to primary care that Drs. Philpott/Kiran and others propose. At their heart, ideas like this are reasonable, make sense and will help improve health care for the general population (I bet you didn’t think I’d say that did you?). They speak to a fairness that just isn’t apparent in the current system. One of the reasons that people pay taxes is so that those taxes can fund health care. How is it fair then, that one taxpayer has a family doctor, and another does not? How is it fair that one quarter of Ontarians can access team based health care, but the rest cannot? And so on.
Well then, what’s the problem and why do I think “Health Care for All” type policies will hurt physicians and patients?
Because I simply don’t believe that our politicians/health care bureaucrats will be able to implement all the work necessary to support this, prior to implementing this change.
Look at the other items I mentioned. Do you really think that the bureaucrats who mucked up so badly will get it right this time? Do you really believe that those bureaucrats are going to provide the admin support, the additional allied health workers, the organizational and structural backing first, before just writing out “everyone gets a family doctor” in the funding contracts?
Not a chance. Zilch. Zero. They will look at the need to invest in teams and say “too expensive.” They will look at the need to add administrative support first and decide that’s not feasible. They will look at the need to build healthcare infrastructure and be confused as to how to do it properly. They will be aghast when they come to the part that says for teams to be successful, they must be physician led. “But I’m the aide to the executive secretary of the assistant to the assistant deputy minister’s attache for the chief regional officer of the Primary Care Branch of the Ministry! I should run the team!”
Then they will come to the part of the policy that says ensure every patient in a geographic area has a family doctor. And those bureaucrats will say “oh that’s easy to do with just some changes and regulation”. And they’ll do just that without any of structural changes needed.
I did some rough calculations for my neck of the woods. Each family doctor in my area would have to take on 200 unattached patients to make this work. The problem is we’re all working at 110% capacity right now. There’s no way we can do that.
So, once “health care for all” comes in what’s going to happen? Physicians will stop doing comprehensive family medicine, myself included. You can only ask a person to work so hard before they get frustrated and quit. Which increases the burden on the remaining physicians, which will cause more of them to quit. And so on.
What’s worse, presenting these policies now deflects from the main issue. Basically, family medicine is no longer economically feasible. Without some immediate stabilization funding, family medicine will collapse. By the time people figure out how to implement “Health Care for All” and reduce admin burden, you won’t have any family physicians left. By introducing the “right to primary care” now, the laser like focus on just what is needed to make family practice economically viable is lost and this hurts everyone, patients included.
I genuinely have a great deal of respect for Dr. Kiran and Dr. Philpott in particular (she was the one who sacrificed her political career to warn us that our Prime Minister was an effete, vacuous ninny who for the sake of all Canadians needs to go back and teach drama classes). But as well intentioned and well thought out as “Health Care for All” may be, now is not the time to talk about it.
Economically stabilize and support family medicine first. Then let’s talk.
NB: This blog originally appeared in Huffington Post Canada on Nov 3, 2015. With the demise of HuffPo it’s being reposted here for future reference.
As someone who had his formative years in the 1980s I can still vividly recall former First Lady Nancy Regan launching the ambitious “Just Say No” campaign. She championed this slogan as part of the “war on drugs.” This “war” was started by Richard Nixon in 1971. He declared that drug abuse was “public enemy number one” and that “the only way to fight this menace was on many fronts.” I can personally attest to having been a true believer in that policy myself, after having done some volunteer work in an emergency department as a teenager.
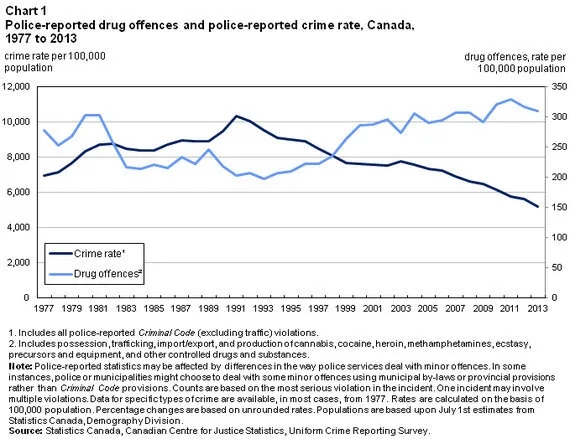
In recent years Canada of course, for the most part followed this policy. In our country, the main technique to fight this war appears to be conviction and incarceration of those caught with illicit drugs. For example, possession (not sale, but possession) is punishable by up to five years in prison. However, what’s clear is that this has failed to help the problem. Data from Statistics Canada (the most recent I could find) shows that while marijuana use in Canada has been relatively constant, the rate of cocaine and other drug use has gradually been increasing since 1977.
The drug trade itself has seemed to grow and is now considered to have a global value of over $300 billion (U.S.) per year. In Canada, as you can see below on this chart from Statistics Canada, drug offences continue to rise, while the total crime rate decreases. So certainly based on this data, it would be difficult to suggest that the “war” has been successful.
As a family physician, I have seen first hand the effects of untreated drug addiction. Far beyond the relatively easy to measure economic numbers, lives have been ruined, families torn apart, some young women forced into the sex trade to pay for their habit and more, are all part and parcel of this terrible disease. Clearly, the goal of any national policy should be to take proven effective steps to reduce the rate of addiction.
The newly elected Liberal government of Justin Trudeau plans to legalize marijuana. To that end, my hope is that Canada can go one step further and focus on what works to reduce addiction rates. While it is clearly counter intuitive to suggest this, it turns out that the best way to do this, is to decriminalize the possession of small amounts of drugs.
While about 25 countries have decriminalized drugs, the best example of how this policy works is seen in Portugal. They decriminalized the possession (not sale, possession) of drugs for personal use in 2001. The offence was re-classified to an administrative offence as opposed to a criminal one, punishable at most by a fine. At the time, may people, myself included I might add, predicted that this would lead to an explosion of drug use, and that children would be targeted, and the nation would decay. As an aside, this rhetoric is similar to what Stephen Harper alleged would happen if we were to legalize marijuana in the last election. However, a review of the results 14 years later suggest that quite the opposite has happened.
Among other benefits, Portugal has seen a reduction in “past year” and “past month” drug use; a reduction in a dramatic decline in HIV and AIDS in drug users, a reduction in crime; a reduction in addicts in prison and a reduction in drug deaths. This has clearly been an extremely successful policy.
So what happens in Portugal when you are caught with 10 or less days supply of an illicit drug? Your case is referred from the Ministry of Justice to the Ministry of Health (a huge shift in and of itself) and you appear before a drug dissuasion committee. You may be fined, but more often are not and you are offered treatment for your addiction, part of which included social re-integration. Their rate of drug addiction has fallen in half since the implementation of the policy.
Ah, but these programs are expensive aren’t they? Surely it would cost a lot to provide this service for addicts. You mean more than the $117,000 a year we currently pay to incarcerate them? Which, as is proven, doesn’t work.
As mentioned, I was a true believer in the war on drugs, but at the end of the day, as a physician, I have believe in an evidenced-based approach. The evidence shows that incarceration doesn’t work, and decriminalization with offers of treatment do. It’s time to ignore dogma and act in the best interests of Canadians. It’s time to end this war.
My thanks to guest blogger Dr. Deepa Soni, an Emergency Room Physician at Credit Valley Hospital. She has written a much more eloquent letter to her MP about the recent tax changes introduced by the federal government, and allowed me to reproduce here as an open letter.
The Honourable Anita Anand,
MP, Oakville,
301 Robinson Street
Oakville, ON
L6J 1G7
April 20, 2024
Dear Minister Anand,
I’m writing to you as a constituent of your riding in Oakville regarding your government’s capital gains taxation measures introduced in this week’s budget.
As an emergency physician for the last 25 years, I and thousands of my colleagues in Ontario, were saving in our medical corporation to be able to fund benefits that many Canadians have available through their jobs: maternity leave, disability, and medical/dental benefits. In addition, and most importantly, incorporation allows us to save for our retirement as we do not have pensions (again, a benefit many Canadians, including government employees and civil servants have as part of their employment). Incorporation was a negotiated benefit that was given by the provincial government in lieu of increasing our fees, with the understanding that the structure would allow us to mitigate some of these factors about our career.
Anita Anand, President of Treasury BoardChrista Freeland, Finance MinisterJustin Trudeau, Prime Minister
When planning for retirement under one set of assumptions, and then finding out that the federal government has moved the goal posts to extract revenue for its budget shortfall, you can understand why so many physicians are bewildered and disappointed by the Liberal government. This would be the equivalent of someone changing the terms of your pension or taking large chunks of it away. For many doctors, this will have profound impacts on their ability to retire when they thought they would.
In addition, as a daughter of first-generation immigrant parents, both of whom were physicians, I am certain you had a front row seat watching your parents work hard to obtain their medical degree, residency, and then establishing a practice. This is not to say that other Canadians don’t work hard: the one thing that makes doctors unique is that our fees are set by provincial governments and our fees have not risen to keep up with inflation. Unlike other incorporated professionals such as accountants, dentists, and skilled trades, physicians cannot increase their fees to make up for rising costs. We are locked into the fee schedule determined by provincial governments (who are always employing cost containing measures to balance budgets). The federal government is turning a blind eye to this important point as it does not fall under federal jurisdiction. Nevertheless, the impact cannot be ignored.
As a corporate lawyer prior to being elected an MP, I’m sure you would not have wanted your hard work and education to be characterized with the words ‘tax cheat‘ if you had been using a legal way to save for retirement. This is the narrative being circulated in the media and it is deeply disappointing. It is noteworthy that MPs receive an annual pay raise (this year ranging $8000-11900), along with pension and benefits. This makes an MP salary one of the highest earners in Canada, with guaranteed income through retirement.
Yet, it is doctors who are singled out as being in the wealthiest 1% and rhetoric implying that we are not doing our part for less fortunate Canadians. We pay into personal taxes and contribute to the economy like everyone else. As small businesses, doctors support the economy through employing staff (nurses, allied health, receptionists etc.), paying rent, and financially supporting many Canadian companies providing support services to our practices (electronic medical records, medical office supplies etc.).
We are also entrusted with caring for the population of Canada in the most sacred way. This taxation measure comes at a time when the medical profession in Canada is suffering unprecedented levels of burnout. Millions of Canadians cannot access a family doctor because they have closed their practises and left (in large part, due to rising costs and fixed fee schedules). Why in an era when attracting medical graduates to do family medicine is a priority, would your government eliminate one of the few advantages that help new grads set up comprehensive practices so they can care for Canadians from cradle to grave? Does your government understand the downstream effect this capital gains taxation will have on patients for decades to come?
From watching media interviews recently, it appears that the federal government’s solution to this is “we will just allow in more foreign doctors“. This is deeply hurtful on many levels: it devalues currently practising physicians who have put in their life’s work to bring excellent care to this country’s patients. In addition, it takes many years for a doctor to acclimatize to the healthcare system in Canada. What happens to patients in the meantime? The solution is not to “throw the baby out with the bathwater”. The solution is to step back and really take in the impact of these actions and the message that has been conveyed to the physicians of this country. I hope your government will rethink this and choose to act fairly regarding incorporation for medical professionals.
Dr. Madura Sundareswaran guest blogs for me today. She’s a community family physician who’s resume is too long to print here. She helped found the Peterborough Newcomer Health Clinic and is a recipient of the CPSO Board Award which recognizes outstanding Ontario Physicians. This article originally appeared on her LinkedIn page.
The day people stop asking this question is the day we have fixed the primary care crisis.
I’m a family physician doing community-based comprehensive family practice in Peterborough, Ontario. I currently work in three different primary care models in our community – fee-for-service, a team-based family health organization, and nurse-practitioner led clinics. All of my colleagues work very hard providing excellent care to their patients.
Despite this, the latest figures suggest that 32,000 people living in the Peterborough region do not have a family doctor.
What does that look like?
A woman in Peterborough notices a breast lump today and is very worried about it. She frantically searches google and reddit to learn that there are no walk-in clinics here. She calls a number late in the afternoon for a local clinic for unattached patients, but all the spots are full for the day. Her options are a virtual doctor who will never conduct a physical exam – but she thinks an exam is important – how will they ever know what this lump feels like virtually? She wants someone’s expertise, she wants reassurance. She decides to go to the emergency department for this problem…but leaves after waiting for 9 hours. She is guilt-ridden as she waits there – she is not as sick as the others in the waiting room. No physician or nurse practitioner will have enough of a relationship with this woman to know that she recently lost her best friend to breast cancer and the impact this has on her illness experience. She is freaking out about this lump…alone.
Or…
A 68 year old male has seen a few pharmacists and virtual family doctor for his hemorrhoids over the last year. He decides that he just has to live with hemorrhoids. A google search says his symptoms are classic for the problem; he’s reassured. As a doctor, I know that this gentleman needs a physical exam but this man cannot find someone to do it. After a few months he winds up in the emergency department with terrible pain – a physical exam very obviously demonstrates rectal cancer. It’s had a year to grow.
Or…
George is a 58 year old man who has never had a family doctor. He has been on Health Care Connect for four years but no one has ever called him to say they have found him a family doctor or nurse practitioner. He is in “perfect health” so he does not need a doctor. He has never had his blood pressure checked, never been counselled on smoking cessation, and has never had bloodwork done. What he doesn’t know is that his Hemoglobin A1c is 7.4 (he has Type II diabetes but too early for symptoms), he has hypertension (high blood pressure – which in its most common form has no symptoms or signs), and his cholesterol is really high. George will probably have a heart attack in the next 10 years. The potential consequences of a heart attack are death. This was entirely preventable.
What we know: attachment to a regular primary care provider (family physician or nurse practitioner) leads to more preventative care, better chronic disease management, and lower rates of hospital admission (ref)
We need a solution ASAP
I eagerly watched as Ontario announced $110 million that will “connect up to 328,000 people across Ontario to primary care teams.” For my community this also translated to a promise for a community health centre (CHC) to connect 11,375 people to primary care. This is much needed but not enough.
Ontario Health Minister Sylvia Jones announcing expansion of primary health care teams
In order to develop a community health centre – a building must be built or set up, policies will need to be implemented, and several primary care providers including physicians, nurse practitioners, social workers, pharmacists, dieticians, etc. will need to be hired. Even if this could be set up within 12 months, where does that leave the other 20,625 in the region without a family doctor? I’ll tell you – scrambling door to door and still knocking asking if anyone is accepting new patients.
But wait! There are other options. A single full-time family physician working in one of Peterborough’s existing family health organizations can roster approximately 1300 patients and join an existing team-based model. We currently have job openings in every one of our five existing multi-disciplinary teams for family physicians. A clinic could be up and running in a matter of weeks. There are family doctors in this community who are very eligible to take on this job – and would likely consider it if they were fairly and adequately compensated.
Learning from British Columbia
I am a firm believer in learning what works and never reinventing the wheel.
In 2023, British Columbia completely revamped its pay structure for family doctors. They paid their doctors better and restructured compensation models – and apparently within a year they got 700 more doing comprehensive, community-based family medicine.
Dr. Ramneek Dosanjh, Past President of Doctors of BC, who called the new funding formula for family physicians in BC a “seismic shift”
I am going to make a few assumptions but I want to illustrate and oversimplify something here.
In the new BC payment model, the pay per full time doctor increased by $135,000/year (assume per full time equivalent). It wasn’t just a pay raise – it involved a few critical changes regarding what doctors could bill for and some restructuring. But the end result was a pay raise.
This resulted in an increase of 700 family physicians (assume full time equivalent) practicing comprehensive family medicine over one year.
Let’s say 1 full time doctor rosters 1300 patients.
If Ontario could get 700 new full-time family doctors to provide comprehensive, community-based family medicine, 910,000 people could now have a family doctor.
The entire rollout for the BC program is budgeted at $708 million over three years but this would include complete restructuring from fee for service care. Ontario already invests over $1 billion annually in interdisciplinary primary care teams and we have a significant head start compared to BC a year ago.
In contrast, Ontario plans to spend an additional $110 million to connect up to 328,000 people across Ontario to primary care teams.
Providing family doctors with the financial support and resources to set up their own practices is the best bang-for-your-buck approach if the goal is patient attachment to a primary care provider.
We need an all hands on deck approach. Support community health centres, nurse practitioner led clinics, but please also support family physician’s practicing family medicine. That is the only way you will achieve attachment for all Ontarians.
Your most obvious solution is pay family physicians better today – so they will hold off retiring for a couple more years and may actually sign on to take a practice.
British Columbia just proved that fair and competitive compensation for family physicians may result in more of them doing it.
Why do I care?
I have been in family practice for five years. I have a roster of patients who have access to a whole range of team-based primary care services – a pharmacist, a social worker, a nurse practitioner, an RPN and multiple other service through our family health team. Every day I get asked if I can take on a friend or family member as they do not have or just lost their family doctor. This simple ask creates a great deal of stress and guilt for me. I know what happens when someone does not have a family doctor or nurse practitioner. They will be sicker, they may die sooner, they will be alone trying to “doctor” themselves.
The moral distress of being made to feel like I am determining people’s fate – giving some people a high standard of care while others are left to fend for themselves will be what ultimately leads to my exit from this profession in this province.Why do I get to give a small handful of people comprehensive team-based care, while the rest (often marginalized, more vulnerable patients) get nothing? It is not fair.
What next?
We are all eagerly awaiting the next negotiation between the Ontario Medical Association and the Ministry of Health.
If we do not see a pay raise for physicians, or worse, we pay them less – everyone in Ontario can accept the reality that they may have a lovely multidisciplinary medical home with a diverse range of primary care providers – but a family doctor probably will unlikely be part of it.
The next time a leader or politician is raving about their new model for care – or pitch a strategy that does not include a family doctor I urge every tax payer and journalist to ask them:
1. Do you have a publicly funded family doctor? (Do you truly understand what it means not to have one? Have you ever had to endure the struggle?)
2. If you are so confident in your plan, would you be willing to give up your family doctor to one of the 2.3 million people in Ontario without one?
3. Why is fair and competitive financial compensation of family physicians not part of your multi-pronged approach?
We are listening to politicians and leaders sell us on an idea of a fully-funded, glorious renovation. Meanwhile the house is on fire. Your family doctors are a dwindling number of people who cannot contain the flames. What are they worth?
Full disclosure: I am a consultant for Medicte, a medical tourism firm that provides high quality, cost-effective medical treatments for ALL health conditions in Turkiye. Contact: info@medicte.ca for more information.
Recently, former Ontario Medical Association (OMA) President Dr. Shawn Whatley wrote an opinion piece in the National Post (later reproduced in the Medical Post) quite correctly rebuking Federal Health Minister Mark Holland for insulting people who consider leaving Canada for medically necessary health care. According to an Ipsos Reid poll, that’s 42 percent of all Canadians. As Dr. Whatley pointed out, this isn’t exactly a new phenomenon. In 2017, well before the Covid pandemic that people like to blame for just about everything, over 217,000 Canadians left the country for medical care. God only knows the 2023 number, but it will most certainly be higher.
Federal Health Minister Mark HollandOMA Past President Dr. Shawn Whatley
Ironically enough, the day after Dr. Whatley’s piece was reproduced in the Medical Post, the Medical Post sent me their daily email which included a link to an article that showed Canadians are waiting even longer for surgical procedures than they were in 2019, and it’s not like the 2019 numbers were any good to begin with. It’s well known that increased wait times result in worsening morbidity and mortality (i.e. the longer you wait, the sicker you become). So it’s no wonder that Canadians are exploring ways to get treatments quickly, even if they have to pay out of pocket. Heck, I’m already on record as saying that I will go to Turkiye if Allah/God/Yahweh forbid I got a serious medical illness.
If you too are exploring medical tourism, here’s a list of things to consider.
How safe is the country I’m going to?
The sad reality is that the world has turned decidedly ugly these past few years. Picking a safe country can be hard. Stories like the one about Americans who went to Mexico for medical tourism and got shot by drug cartels get widely publicized. But there are many unsafe countries in the world. If I was looking at south of the United States, I’d probably limit my choices to Costa Rica and Cayman Islands. There are simply too many economic, political and frankly criminal elements in the rest of the countries south of the U.S.
Even in different continents you have to look at safety first. About 5 years ago a patient of mine of Ukrainian descent went back to Ukraine for a procedure. Obviously would not suggest that now with the war on. So look for somewhere stable.
What is the quality of the hospital I will get treatments at?
No hospital is perfect. But you should at least ensure that the hospital you are going to get care at is accredited by the Joint Commission International (JCI). They are the leading international organization that accredits hospitals and other health care organizations in 70 countries across the world. JCI Accreditation won’t guarantee a successful treatment, but it comes with the assurance that you will be getting appropriate health care.
After ensuring JCI accreditation at the facility you are looking at, then check for references. See if you can talk to people who got care there for their first hand experience.
Get a video consult first.
It’s the 21st century people. Video calls are a thing. If the health care organization you are looking doesn’t offer you the ability to have a video consultation with their doctors, before flying out to their country, well that’s a bad sign. During the consultation, ask lots of questions. Specifically ask about their complication rates and what is covered if you are unfortunate enough to get one. Get a “feel” for the doctor. It’s a big decision, be 100 per cent comfortable that the health care organization you are considering, will be able to take care of your needs.
What’s the Cost?
Obviously, at the end of the day, you are going to have to pay for your treatment. I would, of course, not suggest getting the cheapest possible treatment – because that institution has likely cut a lot of corners to get the price down. But at the same time, I weep for the lady from British Columbia, who, frustrated with the long wait times to see an oncologist, spent over $200,000 (US) on cancer care in the United States. She could have gotten the same treatments for around $70-80K in Turkiye. That’s obviously a lot of money, but still a significant savings.
This is actually why I would recommend you NOT go to the United States for medical tourism. Firstly, they have quite a bit of variability in terms of the care they provide. Some facilities are really good and others……well, some are really good. Secondly, the cost just isn’t worth it. A joint replacement that costs $50,000 US in the United States, could likely be had for $15-$20,000 US in another country.
If you are on a budget, or if you, like many others, are going to take out a loan or dip into your retirement savings to pay for these treatments, that difference is significant.
In Conclusion
While some provinces are making necessary investments in health care, the reality is that improvement in wait times are likely years away. The Canadian public is not stupid, they know this. Only 17% of Canadians feel the health system will improve in the near term.
In the interim, I fully expect the number of Canadian citizens who opt for medical tourism to increase. This can be a safe and effective option for Canadians willing to explore this route, but it is important to do your homework first.
Just me again, your erstwhile, somewhat (but not completely) humble old country doctor. Like last time, I would point out that I am really not your harshest critic. I want to recognize that you have done much for health care infrastructure over the past few years.
For reasons that I cannot fully explain, the previous Liberal regime simply stopped building the necessary infrastructure to help Ontarians. Whether it was new (badly needed) nursing homes, new hospitals, or new teams, the Liberals basically did, well, nothing in terms of infrastructure. To your credit, you’ve reversed that trend and are building facilities we in Ontario need. (As an aside, you seem to like building things a lot!)
Ontario Premier Doug Ford
But all of that building will not mean much in two years (when the next election is – nudge, nudge, wink, wink) if, as projected, over 25% of Ontarians don’t have a family doctor. Yes, you can correctly point out that the decline in family medicine was caused by the Liberals (it truly was – Eric Hoskins was by far the worst Health Minister I personally have seen in my time in health care). You can point out that the Liberals slashed the capitation model favoured by most family docs that started the downward trend. You can also point out that their favoured Deputy Health Minister Bob Bell thought family medicine was so easy he could return to it after over thirty years away:
Screenshot
He even tried to mansplain one of the true leaders of family medicine on how the system should work.
Thx Doc Silvy. I suggest that we need fundamental re-think of highly prevalent, poorly managed conditions. Agree that GP focused practices have cropped up in many of these areas, Sports, MH, PC, Chronic Pain- real issue is lack of programmatic care across province. 1/4 https://t.co/hblPVJqDzX
It’s true Bell and Hoskins were completely wrong. That will NOT matter because by 2026, the general public will say – “well you’ve had 8 years to fix this – you haven’t done enough”. That’s just how politics is, and I think deep down you know that.
You can, truthfully, also say that you are listening to organizations like the Ontario College of Family Physicians or the Ontario Medical Association (OMA) and who continue to go on about how team based care is the future of family medicine and how it can help solve the problem. You may not know this but I was the founding Chair of the Georgian Bay Family Health Team . I happen to believe in physician led team based care.
But here’s the thing. It will take a minimum of five years (if we’re lucky) to build out all those teams. That’s assuming the bureaucrats from the Ministry GET OUT OF THE WAY and let front line family physicians be in charge of the teams. But we are losing family doctors by the week. The people of Ontario can’t wait five years.
There is one thing that can be done now however, to stem the tide, and stabilize the system. You need to give comprehensive care family physicians an immediate, and significant raise. How significant? You will need to give an immediate 35% increase to comprehensive care family docs along with annual normative increases for the next four years. If you think that’s outrageous – I invite you to look at Manitoba’s contract or Saskatchewan’s or British Columbia’s. The competition for comprehensive care family doctors has increased significantly, and Ontario is falling behind.
I can pretty well guess what your “advisors” are telling you. They will say you are in arbitration with the OMA, just promise to abide by the result. Honestly, I do believe you will abide by the result, both this year and next.
But…
Arbitration will take months this year, and months if not a year next year. Frankly, I doubt that the OMA, despite their strong words, will advocate for an increase of the amount necessary for comprehensive family medicine (hopefully I’m wrong).
I have absolutely no doubt that the Arbitrator, William Kaplan, will give a raise to family docs, especially after the recent award to nurses. But if the raise isn’t enough, you going out to the general public in two years and saying “we honoured the arbitrators rulings” – will make zero difference to the close to five million people who won’t have a family doctor. They will still blame you for not having been pro active.
William Kaplan, Chair of the Arbitration Board
Listen, I’m on the conservative side of the political spectrum. I’ve always voted for the Conservatives in every provincial election since I was eligible to vote. I live in Simcoe – Grey which is one of, if not the most strongly conservative ridings in Ontario. Heck, in the early 1990s we were the ONLY riding east of Manitoba to vote for a Reform Party MP.
I’m telling you that most of the voices on the ground are really upset about the lack of family doctors. We have about 7,000 patients without a family doctor in our area last I heard. It’s true that when asked who they will vote for in polls, they, like most recent polls, say they’ll vote conservative. However, they always add “I guess, there’s nobody else out there”. That softness in your vote is a problem, and that softness doesn’t show up in the poll numbers.
Listen, I want you to win the next election. I personally think the NDP would be a complete disaster. I have no faith the Liberals, who showed just how much they hate doctors, have changed their tune. But in order to do that, you’re going to need to bite the bullet, and stem the haemorrhage of family docs.
Go to tell your negotiations team to offer up a deal that strengthens family medicine. Mask the increase with things like retention bonuses (like Manitoba) and matching RRSP payments (like BC) and other methods (paid admin time, paid supervision of team members and pensions would be nice). But get it done ASAP.
Otherwise, I genuinely think you will be in more trouble than you might be led to believe by your handlers in 2026.