The Canada Health Act (CHA).
Written by former Federal Health Minister Monique Begin, and passed into law forty (!) years ago, it transformed health care in Canada, and in many ways transformed the country.

Viewed as sacrosanct by many pundits, it has now reached a status amongst politicians where health care is widely viewed as the “third rail” of Canadian politics. To question the reverential status of the CHA is to invite political ruin, and to be forever labeled as un-Canadian. I guarantee that I will be accused of being a proponent of “two-tier American style health care” simply for suggesting that the CHA should be reviewed.
Yet review it we must, because the reality is that a LOT has changed in health care in the past forty years. The CHA was written before the explosion of medical knowledge we have experienced. To expect it to still be appropriate is naive at best, willfully neglectful at worst. My much smarter friend Dr. Mathew pointed out: The CHA was written when health care was “episodic”. You got sick, you went to the doctor. You usually had a small co-payment. You got treated for the illness you had.
But since the CHA, health care has been massively transformed to focus on prevention. Whether with the explosion of screening tests for cancer, a focus on control of chronic illnesses, or a recognition of the benefits of being able to afford prescription medication, health care is different than 1984. In a big way. This is why the government is again promising pharmacare.
While there will always be a paper, or plan or policy on how to improve health care, very few people have the courage to address the root cause that is stagnating and impeding change, namely the CHA.
For example, Dr. Tara Kiran (Fidani Chair of Improvement and Innovation in Family Medicine at the University of Toronto) had a four part series on health care in the Medical Post where she compared Canada to Denmark. She looked at how Denmark organized their family doctors, how they pay physicians, their EXCELLENT health IT system and so on. All of which is wonderful and really should be emulated here in Canada.
Similarly, former federal Health Minister Dr. Jane Philpott has been in the news a lot with her new book “Health Care for All” in which she talks about the “right” to have a family doctor. In an interview with the Medical Post she glowingly references Norway, and how they build in health care infrastructure, much like they build schools, when planning developments. A lot to like about Norway’s health care system.


But, did you know that Denmark has a parallel private health care system (despite their high taxes) that allows faster access to care along with access to more specialists and other services? Did you know that in Norway, you actually pay for you health care at the point of service until you reach your deductible (2,000 Krone, about $250 Canadian)?
You mean Drs. Kiran and Philpott never mentioned that these countries whose health care systems they have been talking up had defacto co-payments for medical treatments (gasp!) and parallel private health care (gasp!). Gee, I wonder why….
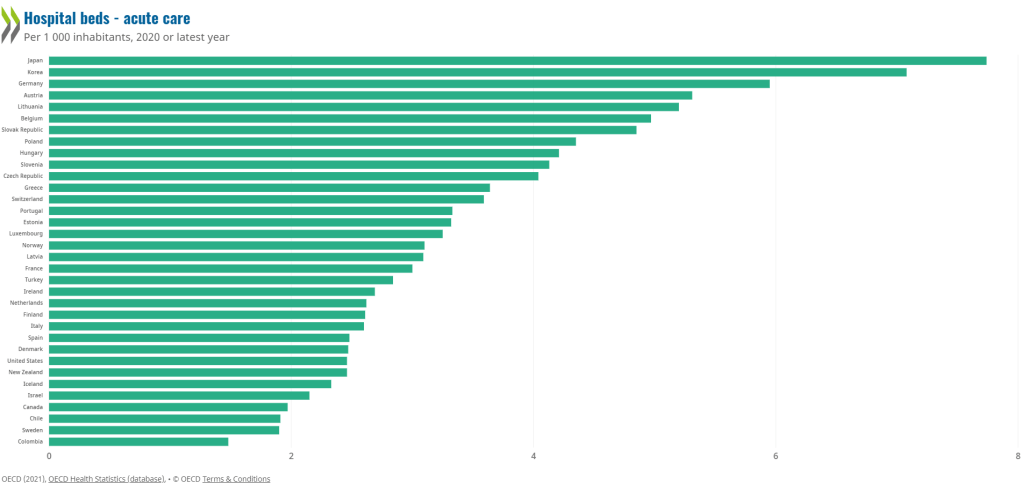
Here’s the thing. EVERY single country that has a better health care system than Canada’s has TWO main features:
- A universal health care system that is funded by taxes
- An element of private care, usually some combination of a deductible for taxpayer funded services, and, a private system.
To deny the above is simply to deny the facts. To cherry pick what other countries do and to think we can do it here in Canada without also recognizing that much of what they do would contravene the CHA is naive at best, and disingenuous at worst.
Canada had a health care system that was ranked very highly in the mid-1980s. Ontario used to boast of having the “best health care system in the world”. It’s undeniable that since the CHA, health care in Canada has deteriorated markedly when compared to the rest of the world. This is not a coincidence.
What can be done? I believe the CHA should be changed to allow the federal government to have strong controls to ensure a fair universal health AND pharmacare program that functions like a true insurance plan (yes that means deductibles). It should also empower the feds to enforce a Canada-wide health IT system that allows patients to access their own data.
Why deductibles? Why not have the taxpayers pay for everything? Because without them you take away the responsibility for using a service properly. People feel as if it’s something they deserve as opposed to something they have a joint responsibility to manage and care for. By making deductibles illegal, the CHA has created a society of entitlement, instead of one of empowerment.
If you think I’m un-Canadian for suggesting that there should be a deductible on taxpayer funded health insurance, then I would ask that you be fair about it and also call the guy who said this un-Canadian:
“I want to say that I think there is a value in having every family and every individual make some individual contribution. I think it has psychological value. I think it keeps the public aware of the cost and gives the people a sense of personal responsibility.……there is a psychological value in people paying something for their cards……… We should have the constant realization that if those services are abused and costs get out of hand, then of course the cost of the medical care is bound to go up.“
That fellow? Why none other than the “Greatest Canadian” himself, Tommy Douglas.
Health care in Canada is at crisis. Patients are suffering terribly. One third of physicians are thinking of leaving the profession in then next two years, just when Canadians need them most.
A crisis demands you look at all options. The first step is to revisit the CHA.