Another in a weekly series of brief snippets of health care stories that bemused, intrigued and otherwise beguiled me over the past week along with my random thoughts on the matter.
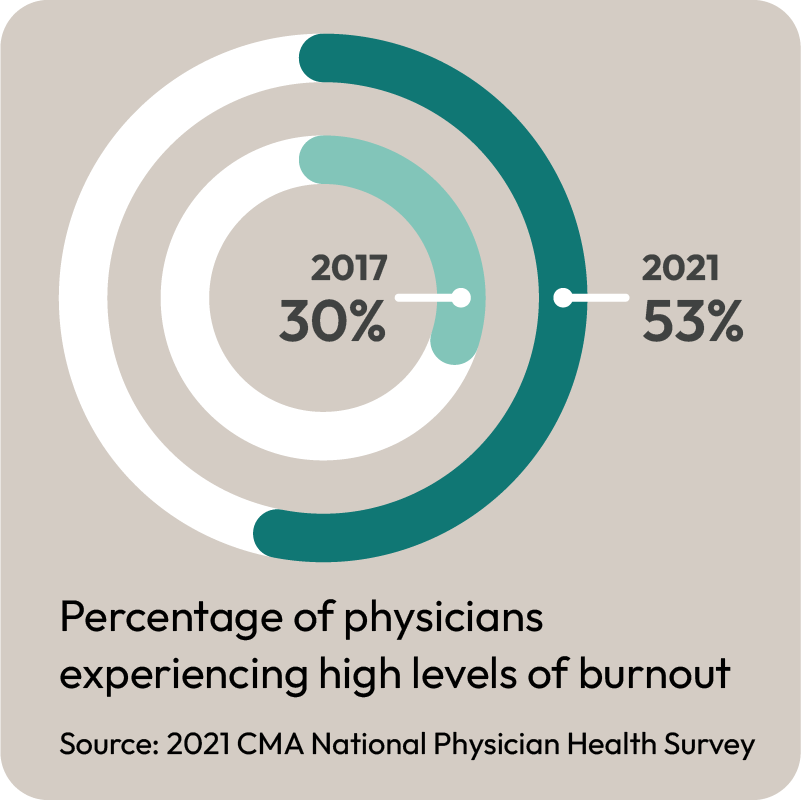
My thoughts: Kudos to Dr. Giles for talking so openly about this. Alarmingly few of my colleagues are willing to talk about burnout and how the system is affecting them. Instead they suffer in private, and that’s not healthy for them OR the patients they serve. It’s an important story that needs to be told over and over again.
Item: “Involuntary medical treatment” for people with addiction issues seems to be all the rage. A great article in the “Conversation” shows that this won’t solve anything, and in fact will make things worse.
My thoughts: I really can’t believe we are even discussing this. It has been well known for…..well forever, that people will not get better unless they want to seek help. We have to focus on making seeking help easier, not forcing them.
Item: The always excellent Dr. Katelyn Jetelina, who most of my colleagues know as a superb voice of reason and information during the height of the Covid pandemic, writes about her feelings now that RFK junior has been nominated to lead Health and Human Services in the United States.
My thoughts: My heart goes out to her and all the hard work staff who have tried keep us all safe during the pandemic. They deserve better.
Robert F. Kennedy Jr., a leading American Anti-Vax conspiracy theorist, now tapped to head Health and Human Services in the United States
Item: TV Ontario had a segment suggesting that foreign trained physicians could help tackle Ontario’s physician shortage.
My thoughts: I’ll shout it out again, we already have enough family doctors in Ontario who are already licensed to practice medicine in this province and are familiar with the Ontario Health Care system. The number is approximately 6,000 or so (see the graphs in the linked blog for details). Can we just not make it easier to practice family medicine instead??? If we can get even 1/3 of those doctors already in Ontario to start a practice, we would end this crisis.
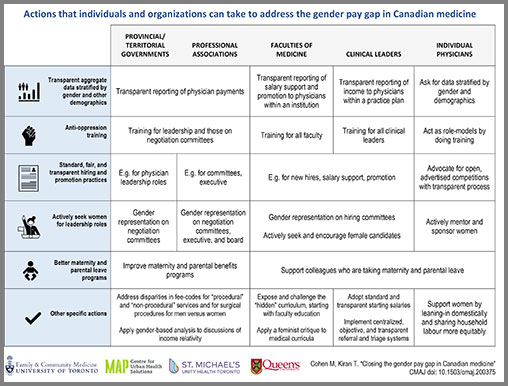
My thoughts: One of the best accomplishments of the OMA Board when I was on it was to publish the gender pay gap report. It was arguably too late, but I believe we were the first PTMA to discuss this and to use that as a basis for future negotiations work. While I’ve had some issues with how negotiations have been handled since, I am quite comfortable in saying that positions of the OMA in negotiations would take this into account and that there is likely to be funds demanded to narrow this gap. The blame for the fact that there has been no progress on this lies mostly at the feet of the Ministry of Health. We don’t have an agreement yet on how to divide the arbitration award – and that means the Ministry is not responding to OMA proposals that would close this gap. Shame on them.
My thoughts: The National Health System (NHS) in Britain is under fire for the fact that it too tried to replace the work done by fully trained physicians, with staff who were likely well intentioned, but had less qualifications. It turns out there is significant risk to this, and likely a markedly increase cost in providing health care. The article “My wife died because the NHS used cheap labour” should be, in my opinion, required reading for any politician/health care bureaucrat who thinks they can provide better care by using less trained people.
That’s all for this week. Back next week (probably) with more.
Bureaucratic vertigo in Ontario’s home care system, exacerbated by ineffective reforms and rebranding, has led to chaos and service stagnation, necessitating genuine engagement with frontline providers for meaningful transformation.
Dr. Merritt Cade (not their real name) is a concerned and experienced Ontario physician familiar with the current crisis in home care. Dr. Cade is worried about potential blowback from this blog that will affect their patients and so this blog is posted under a pseudonym.
Vertigo is a sensation where one perceives movement that isn’t happening. In the realm of healthcare administration, a similar phenomenon occurs—bureaucratic vertigo—an organizational dizziness that mimics change but leaves structures and systems untouched. Nowhere is this more glaring than in Ontario’s home care sector, a pivotal yet neglected component of our healthcare system.
In 2023, amid promises of reform, the Ontario government introduced Bill 135, the “Convenient Care at Home Act,” envisioning a streamlined home care service managed by Ontario Health atHome (OHAH). OHAH itself was to now be brought under the umbrella of Ontario Health, the implementation arm of the Ministry of Health. Hopes were pinned on this transformation bringing ease and efficiency. However, the reality has been a déjà vu of previous cycles of centralization and decentralization of health care structures, with patients and families shouldering the consequences.
Nowhere is the bureaucratic vertigo more evident than in the successive re-branding of home care over the last 8 years from “Community Care Access Centres (CCAC)” to “Local Health Integration Networks (LHINs)” in 2017 to “Home and Community Care Support Services (HCCSS)” in 2021, to the latest iteration, “Ontario Health atHome (OHAH)” in 2024. Meanwhile, regardless of the name used, the services provided by the home care system remained untouched.
OHAH’s own front-line staff, the beleaguered Care Coordinators, were also caught completely off guard as rules regarding medications and catalogues of supplies changed overnight. Care Coordinators are the quarterbacks of the home care system, matching services to patients’ needs. What OHAH and Ontario Health did was akin to completely changing the playbook on their quarterbacks and teams, with sadly predictable results.
Despite all this, however, home care holds immense potential to address systemic challenges, from reducing ER congestion and the alternate level of care logjam to facilitating dignified end-of-life care at home instead of in hospitals. What is required is not another bureaucratic shuffle, but genuine engagement with those who understand home care’s nuances best: frontline providers. It is they who hold the practical knowledge necessary for meaningful reform.
The path forward demands that decision-making authority be shared with these healthcare professionals. Their experiences can inform policies that work in reality, not just on paper. This means abandoning the “bureaucrat knows best” mentality and embracing trust and collaboration. It means abandoning committees struck merely to check a box that says that frontline professionals were consulted when, in fact, their concerns do not meaningfully contribute to decisions made.
Furthermore, the status quo must not define future transformations. Further substantial changes to home care delivery, this time relating to the supply of equipment such as hospital beds, wheelchairs, walkers and other essential aids, was planned for rollout in October but has been delayed until January. Without a change in approach, we should expect similar upheaval when this takes place. Past failures demonstrate that superficial organizational changes do not equate to operational improvements. Genuine progress relies on a foundational renewal of leadership and strategy, prioritizing empathy, accountability, and proactive stakeholder engagement.
If we are to lift Ontario’s home care from its current crisis, change must be substantive, rooted in the insights of those who deliver care day-in, day-out. We must move beyond the spectre of bureaucratic vertigo and commit to sensible, informed solutions that truly benefit patients and families across the province. By trusting, listening to and involving the frontline, we can stop the spin and start the real work of reform.
Another in a weekly series of brief snippets of health care stories that bemused, intrigued and otherwise beguiled me over the past week along with my random thoughts on the matter.
Item: New reports show that marijuana use is linked to thinning of brains in adolescents.
My thoughts: It’s not just adolescents. And it’s not just brains. I’ve seen a marked rise in people with significant mood issues ever since marijuana was legalized. There has also been a significant rise in people with stomach/bowel issues in my practice that all other tests turn up negative for. Patients with these issues are invariably marijuana users and the blunt reality is they won’t get better until they stop. I continue to be in favour of decriminalizing marijuana and other illicit street drugs if and only if we do it the way Portugal did it and not the haphazard way it is being done in Canada. But we really need to re-think the full on legalization of it.
Item: A survey in Medscape showed that there were two factors critical to reducing family medicine burnout. First would be to reduce the Electronic Health Record burden, particularly the number of times family physicians have to chart from home. Second would be to build stronger physician/nurse teams. Crucially, the teams need to be led by the family physician and NOT a bureaucrat or some other team member.
My thoughts: I hope this finally gets the Canadian Medical Association (which despite over $2 billion dollars in their bank account is amazingly growing increasingly irrelevant to front line physicians) to SHUT UP ABOUT SICK NOTES ALREADY. That’s not going to solve burnout (even though I like every other doctor hate doing them). To paraphrase a political slogan – “It’s the Electronic Health Record, stupid.” My second thought is that I remain extremely concerned that while I do feel Dr. Jane Philpott is well intentioned in her new role (to lead a primary care action team) – the bureaucrats at Ontario Health will sabotage her. They will see “teams help”, then create teams that have the assistant to the secretary to the aide to deputy minister’s attache for the Primary Care Secretariat’s deputy vice president run them. That will be a disaster. Teams need to be led by family physicians. Full stop.
Dr. Jane Philpott, head of the new “Primary Care Action Team” designed to give everyone access to primary care in 5 years.
Item(s): The family physician crisis in Ontario continues to worsen. Tillsonburg lost four family physicians. Wallaceburg is launching a large physician recruitment program to deal with their shortage. Brantford is taking a more hands on role to get more family physicians. Brockville is hiring a consulting firm that employs former health Minister George Smitherman to help tackle their shortage.
My thoughts: It’s sad that we are in a seeming “Hunger Games” of one community fighting another for the precious resource that is a family doctor. If only someone had warned people a crisis was coming. Oh, right.
Dr. Nadia Alam, who, like others, warned that the crisis in family medicine (and health in care in general) was coming ten years ago, and was ignored by governments.
Item: Premier Ford promises to correct the mistakes at Ontario Health at Home that led to a large amount of suffering for patients. He also stated that the people who “messed this up” will be “held accountable”.
My thoughts: I’ll believe it when I see it. When I wrote about mismanaged bureaucracy in health care (back in 2015!) I pointed out that no decision seems to get made by bureaucrats without continuously “circling back” to one committee or another. The reason I’ve discovered, is because this way, no individual gets blamed for (the very many) bad decisions made in health care. I’ve yet to see a health care bureaucrat fired – and I’ve met many who deserved to be. I really hope that the comments by Premier Ford signal a return to the old Doug Ford who promised to end the “gravy train” and famously said:
“What drives me crazy is when you have a supervisor in government, and they report into 12 other supervisors. That’s unacceptable.“
Doug Ford, Premier of Ontario for almost 7 years, and the gravy train in Ontario Heath continues unabated
Item: Male doctors are working less hours in a week than they used to. They are still working more than the average Canadian worker, but there has been an unmistakable decrease in how many hours they work
My thoughts: Finally! Proof that men are getting smarter! There’s more to life than work, and good for the younger docs – all of them – for seeking balance in their lives.
Item: A young Ontario mother died of cholangiocarcinoma (cancer of the gall bladder), after encountering multiple road blocks getting a new treatment (Pemigatnib) approved for her.
My thoughts: This story is absolutely infuriating and encapsulates what is wrong with our health care system. Look, there is no guarantee that she would have survived if she had gotten the treatment (it’s an awful cancer she had). BUT – look at all the regulatory agencies involved in getting the drug approved. Health Canada approved the drug in 2021. But the Canadian Agency for Drugs and Technology in Health said the evidence wasn’t clear. (So why then did Health Canada approve it?). Furthermore there are multiple provincial drug agencies involved, which means she could have gotten it had she been a resident of Quebec, but not Ontario (two tier medicine anyone?). It’s the bureaucracy and double speak from having too many agencies involved that angers me greatly. A wholesale streamlining of the process for medication approvals is desperately needed.
That’s all for this week. Back next week (probably) with more.
Another in a weekly series of brief snippets of health care stories that bemused, intrigued and otherwise beguiled me over the past week along with my random thoughts on the matter.
Item: An article in the College of Family Physicians of Canada Journal suggests that “recycling” physicians would help address family physician shortages. This includes “Physicians who have had successful careers in general surgery, emergency medicine, family medicine, hospitalist practices, and other specialties…”
My thoughts: Sigh. I get that the Journal is trying to be open to all views to stir discussion. I get that we are in a family practice crisis in all of Canada right now and looking at unique ways of helping. But seriously – you want to turn a retired general surgeon into a pseudo family doctor? Do you realize just how much you are denigrating family physicians by writing that a good chunk of their jobs can be replaced by people who haven’t done the residency? Some ideas belong in the trash heap and this one deserves to go there. Comprehensive care family physicians CANNOT BE REPLACED by anyone other than another properly trained comprehensive care family physician.
Item: It seems that Quebec is looking to find ways to force doctors to stay in the province and work in their public health system. They are even willing to as far as considering to use the Notwithstanding clause in the Constitution (which they would have to, as their initial position impinges on freedom of movement/assembly to make this happen).
My thoughts: It really does kill me to use Star Wars memes instead of Star Trek ones (really and truly). But once again, for this issue – I’m going to quote Star Wars character Princess Leia:
I honestly don’t know what to do with politicians anymore. There is ample, repeated, overwhelming evidence that whenever they pick fights with physicians, they inevitably lose and health care suffers. And yet they keep doing it.
Item: Dr. Corli Barnes (who I was honoured to have as a guest blogger) wrote in McLean’s Magazine (cover story no less!) about why she moved to Madoc, Ontario and the incentives they provided. I understand she took less than what is listed in the article’s headline, but there were incentives.
Dr. Corli Barnes
My thoughts: I’m happy for Dr. Barnes. I’m happy for the people in her community as well, as they are going to get healthcare from a dedicated family physician and their well being will improve as a result. But I really do wish that our system was no so fragmented and that all communities could offer a consistent level of support to their family physicians.
Item: Premier Doug Ford told patients with minor illnesses not to go to the ER. In response, Drs. Drummond and Venugopal had an op ed where they point out that the Premier is not qualified to determine what is an Emergency.
Dr. Allan DrumondDr. Raghu Venugopal
My thoughts: This will surprise some of you who know that I personally favour the Tommy Douglas model of health care, which supports user fees to dissuade misuse of the health care system. However, that is frankly up to the patients to decide for themselves. Drs. Drummond and Venugopal are correct in saying that politicians are not qualified to hand out medical advice, and should not be saying stuff like this.
Item: A study out of Michigan suggests that more virtual care will not lead to more unnecessary testing. A huge concern has been that if you cannot see a patient in person to assess this, a physician would be more likely to order a test “just to be sure”. This study suggests no.
My thoughts: I think the big flaw of this study is that it looked at patients who were in existing practices getting virtual care from their own physicians. There is a HUGE difference between getting care from your own physician virtually, or getting it virtually from someone you have never met before on some fancy looking app. The two are not the same and it would be very interesting to see how many unnecessary tests are done when there isn’t a pre-existing physician/patient relationship.
Item: Amina Zafar had an excellent piece in the CBC writing about how poorly managed your medical information is. She builds on the story of Greg Price, an unfortunate 31 year old who died of testicular cancer, when he probably shouldn’t have. She writes how this mismanagement of health care information is common in Canada.
My thoughts: Yes, yes, yes, a thousand times yes. As far as I’m concerned, the mismanagement of health IT should be the number one issue to be addressed in health care. It creates countless inefficiencies in our health care system. It creates all sorts of admin burden. It leads to much higher expenditures and duplicate testing. This needs to get fixed ASAP.
Item: The Ontario Medical Association (OMA) announced that nominations are open for their annual election periods. Up for grabs are four Board Director positions and many other District and Section positions.
My thoughts: Physicians in Ontario desperately need a strong OMA. The only way that can happen is if front line physicians stand up and take positions. I’ll be frank (and will offend a bunch of people) – but when I was on the Board there were too many Board Directors who clearly were in it for their own self interest and were not thinking of their colleagues. The same could be said for some other elected reps. We will get the OMA we deserve, but only if front line docs take a leading role.
I’m honoured to have Dr. Mark Linder guest blogging for me today. I first met Dr. Linder during our time advocating against Dr. Eric Hoskins unilateral cuts to health care. He’s exceptionally well spoken and articulate . He’s a former ER doctor and now full time family physician and clinic owner. His other claim to fame is that got fired from the Kaplan MCAT teaching course after one session – which apparently was a first.
I just wrote this in a flurry this morning. I see stupider and stupider proposals from the government and from newspaper editorials. I see our new grads learn from their teachers that they need to stay away from this job. I then see the domino effect this has on recruitment, job satisfaction and reinforced by absurd government initiatives to save the system. I watch the OMA get pulled in every direction to try and please everyone. So apologies in advance -this is just my take really-and mostly to get it off my chest-not that it will lead anywhere. So thanks for reading.
The Family Health Organization (FHO) is what saves family medicine. It has done it before and it can do it again.
In 2006 something unprecedented happened. It hasn’t happened before or since. And perhaps we didn’t quite appreciate how unique it was. The provincial Liberal government, under Dalton McGuinty and Health Minister George Smitherman, introduced an upgraded payment model for Family Medicine. It built on the existing capitation based Family Health Network (FHN) model to enhance it.
Former Ontario Premier Dalton McGuintyFormer Ontario Health Minister George Smitherman
What was so unique about this? It stands out as one of the only times a government has thought beyond their 4 year term to the ultimate health of their population as well as their economy down the road when they may no longer be in power. Sure, it was going to make them look good if everyone got a family doctor out of it-but it was a big expensive risk, a risk based on an assumption that family medicine was critical to the system, AND that practitioners need to be paid fairly for their work if they wish to retain these doctors in the future. A different time to be sure!
It worked. Look at the stats from 2008 to 2018. Look at how many Family Doctors gladly embraced the new system. Look how the number of orphaned patients dropped.
The system had flaws. I mean this was the second iteration of what was described as an experiment. The “outside use” enforcement rule made little sense in most cases. The calculation of capitation payments wasn’t always a fair representation of how much work it took to look after the patient in front of you. Certain “in the basket” fees were bizarre and should never have been part of the package. Doctors were actually more incentivized to send people to the ER over a walk in clinic!!! But all in all, it was a great innovation, a great idea, and saved family medicine. It also, no doubt saved the province millions in treatment dollars and ER visits as family doctors made themselves available to look after patients.
And then, In 2015 Kathleen Wynne and Eric Hoskins, the health minister at the time, effectively shut down enrollment in FHOs And that was the beginning of the end. I presume they just wanted to control the immediate budget – paying for family medicine up front meant huge savings down the road. But it resulted in a pretty big chunk of budget going out the door NOW. And the Wynne liberals didn’t have a health care crisis, didn’t heed the warnings that we as physicians laid out pretty starkly at the time, and decided, nah, we’ll just “pause” the experiment.
Former Ontario Premier Kathleen WynneFormer Ontario Health Minister Eric Hoskins
Which they did. And the fall out was obvious. As a clinic owner and a family doctor, I had a front row seat. The residents and new grads had all been trained in the new system, and now were unable to access it. If they wanted to work, they’d be taking a tremendous risk setting up a clinic in a Fee For Service environment using a Schedule of Benefits that had failed to keep up with inflation for 20 years. They were screwed. The aging Family Doctor population continued to retire at a predictable rate, and the aging population continued to get more desperate to find doctors with increasing difficulty.
By the time the FHO’s opened up again in 2021, it barely mattered–The reputation of family medicine among new grads had been thrashed for 6 years. With the new rules, new grads would have to gather 6 like-minded individuals (instead of just 3 like in the old days), or find a bigger FHO that was already established and could fit them in. Not so easy. Opening up your own shop had become increasingly more expensive with post pandemic inflation, so the debt would be crippling just to get started if you wanted your own clinic. And these are graduates who already had a huge amount of debt coming out of school.
Couple this with the insane increase in administrative burden as we become more and more efficient at having hospitals and labs forward us copies of paperwork. In theory, amazing, in practice hugely burdensome, time consuming and unpaid. Arguably, if the FHO rates had increased at the level of inflation, there’d be no complaints about this additional work. But the FHO rates had more or less remained static relative to the cost of doing business. Still better than FFS, still paid a lot less than the actual market value of doing the job as proven by the lack of uptake that continues today.
The thing is: The FHO is still the answer. It absolutely needs some significant tweaks. The rates need to go up. The outside use concept needs to go. Minimum size and shared EMR requirement needs to be softened so that smaller groups can join together in nearby geographic areas. Some sort of separate funding will be essential to help clinic owners to keep up with inflation. But it still achieves by far the best mix of physician autonomy, clinic management, and long term government savings. And it’s evidence-based! We have a recent history we can look back on to demonstrate efficacy!
Other solutions, such as having lesser-trained individuals diagnosing and managing patients give the appearance of short term gains at a huge future cost as more referrals to specialists are made and more referrals to the ER are made. Another concept of having government run all clinics is clearly so expensive as to be dead at the gates-Doctors currently pay for rent, administration and their own retirements out of their incomes. It’s not great for us, but it’s a heck of a lot cheaper for the taxpayer to do it that way, and simply pay the doctors more.
I recognize that my FFS colleagues are not helped at all by an enhancement and advocacy for the FHO approach. And I’m sorry. I obviously think there’s a lot of work that could be done to improve FFS rules and individual payments. No doubt.
But we actually have the evidence that the FHO saved family medicine when it was introduced. It was stunningly effective, and if nursed back to health, will absolutely work again.
Another in a weekly series of brief snippets of health care stories that bemused, intrigued and otherwise beguiled me over the past week along with my random thoughts on the matter.
Item: AI is now inventing things no one ever said. It turns out that AI can “hallucinate” (no really, that’s what they are calling it). Apparently the AI invents commentary that includes things like racial comments/violent rhetoric (!) and even medical mis- diagnoses.
My thoughts: My group is actually looking at AI to help with our Admin burden. While the technology shows promise – this is a useful reminder that we should all read what software generates before logging off. You will probably still save some time, just not as much as hoped.
Item: A new lung cancer vaccine that uses mRNA technology is entering trials. Somewhat ironically, this is what mRNA technology was being studied before the COVID pandemic, and its use for the COVID vaccines. The technology shows great promise to greatly reduce the side effects of cancer treatment, and provide more targeted therapy.
My thoughts: The “vaccine” term is probably going to need refining, because it’s not really preventing lung cancer (which is what most people associate with the term vaccine). Additionally, social media is still awash in mis-information about mRNA technology. So probably better to avoid that term. But at the end of the day I would agree what we are really in a remarkable time for cancer therapy with so many new treatments available. (Still better not to get cancer of course – so if you do smoke – quit!).
Item: Dr. Elaine Ma, a physician who went over and above the call of duty to organize mass vaccination clinics in the Kingston area at the height of the Covid Pandemic is asked to pay back the billings generated during those clinics. (Note I did not say income – Dr. Ma would have used a good portion of those billings to pay staff, supplies and other overheads).
My thoughts: I’ve been (frequently) told I’m too hard on bureaucrats in health care. That I come across as somewhat insulting and “un-presidential” when I complain about them. And every time I think to myself “I really need to take a deep breath and be hard on the problem, not the people” – along comes yet another example of rigid bureaucratic thinking and frankly bureaucratic stupidity that I wind up reverting to my old habits. I will say this, the residents of the Kingston area are a whole lot better off because of Dr. Ma , and the sooner the OHIP bureaucrats get this, the better. As for the OMA’s silence on the matter, it’s pretty disappointing.
Addendum: after writing this blog the OMA has confirmed that they have been helping behind the scenes. I’m glad to hear that they have been helping Dr. Ma, but I would state for the sake of their members that they need to be SEEN to be helping….
OMA Board Chair Dr. Cathy Faulds, who has been silent on Dr. Ma’s abhorrent treatment OMA CEO Kim Moran, also silent on Dr. Ma’s abhorrent treatment
Item: The Registered Nurses Association of Ontario blasted the government for not embracing nurses as a central to solving the primary care crisis.
My thoughts: I admire the RNAO for advocating for their members (no really, that’s kind of what a member organization is supposed to do). They’re wrong of course. Using Nurse Practitioners to replace physicians (as opposed to complementing them) will only massively drive up the cost of health care and worsen outcomes. But unlike certain organizations- see above – the RNAO stands up for its members.
My thoughts: It’s always awful to see children sick, and as clinicians we should be on the look out for this. BUT – thankfully the vast majority of cases appear to be mild, and if treated appropriately people are recovering. They may have a persistent cough for several weeks – but they are getting better.
My thoughts: A good friend of mine says it much, much better than I could. “We need the political leadership to step beyond name calling and giving token titles to people to win an election. If you want this province to thrive, rebuild and lead Canada again, it requires more than what we have seen for 20 years from ALL political parties .”
That’s it for this week’s Sunday Snippets. As mentioned above, watch out for a really superb guest blog tomorrow on how to fix family medicine.
I was away last week but I’m back with another in a weekly series of brief snippets of health care stories that bemused, intrigued and otherwise beguiled me over the past week along with my random thoughts on the matter.
My Thoughts: Alberta is kind of a funny province. There are some very strange goings on with their health care policy. But it can’t be denied that despite all of that, if you provide incentives to attract younger physicians it will help. Having said that, it can all be easily undone if they don’t get on with it and implement the compensation for family physicians they promised, and for some reason appears to be delayed.
Danielle Smith, Alberta PremierExecutive Committee of the Alberta Medical Association
My Thoughts: What’s that you say? You mean ensuring that physicians have peace of mind about their retirement might actually help recruit (gasp!) and even retain (double gasp!!) physicians? Who would have thunk it?? In all seriousness, given the way the Federal Liberal government of our effete Prime Minister really screwed physicians with the recent tax law changes – this is a necessary move and I hope will get copied by all provinces. It really will help improve morale and reduce some of the burnout.
Nova Scotia Premier Tim HoustonDr. Gehad Gibran, President, Doctors Nova Scotia
Item: John Richards and Tingting Zhang, from the CD Howe Institute wrote an op-ed in the Financial Post encouraging more use of nurse practitioners since they can “do almost everything an MD can”.
My Thoughts: El Toro Poo Poo. (This is a PG rated blog so that’s all I could get away with). I work with Nurse Practitioners and I have seen them help patients and I firmly believe they have a role in health care. But that role is not to replace physicians. The studies that show they can “do almost everything” are done based on what scope of practice suggests they can do. The blunt reality is nurse practitioners drive up costs and worsen care if used in settings as these characters suggest. The studies that show that NPs are cheaper ONLY look at the actual income an NP gets and compare it to a physicians income, as opposed to looking at the work that is actually done/number of patients seen/and number of tests ordered. The FP article isn’t even fit to be used for toilet paper.
Item: The crisis in Home Care supplies, first reported by Avis Favaro on X (formerly Twitter) continues. Home care nurses are reporting heartbreaking stories of patients buying their own supplies on Amazon since home care couldn’t provide them. Dr. Drew Moore and Dr. Hal Berman should be lauded for going public with their concerns. (I’ve met both of them and they are both mensches).
My Thoughts: I’m old. I’ve seen a lot of government screw ups in my time, especially in health care. But I have yet to see bureaucrats who screw up be truly held accountable and fired. Ever. They just get shuffled off to some other department. It it too much to ask that if someone makes a mistake at their job (and this is a BIG one) they get held accountable?
Avis Favaro, Health JournalisDr. Drew Moore, Palliative CareDr. Hal Berman, Palliative Care
Item: Quebec is attacking family doctors for some reason. First they suggested they would link people to non-family physicians for care and even remove patients who were “healthy” from their own family physicians. Then they presented erroneous data suggesting that family doctors basically don’t work hard enough.
My Thoughts: There are 9 other provinces and 3 territories that would love to have these doctors.
My thoughts: Unionization of physicians is going to happen eventually. Whether through the long gestating Charter Challenge (yes my Ontario peeps – it is still working its way through the courts) or some other mechanism. The younger physicians clearly seem to want this model of representation and at some point in the not too distance future, physicians will be unionized.
My thoughts: My thanks to Am640 News for interviewing me on the topic, and my thoughts on this can be heard below. (This short version – this is populist rhetoric that will do nothing to help with the health care crisis):
That we have a family medicine crisis in Ontario is indisputable. That the numbers of family doctors leaving comprehensive care family medicine continues to rise and is expected to leave over 4 million people without a family doctor in the next couple of years is irrefutable. That the need to recruit and retain comprehensive care family doctors has never been more urgent especially as competition from provinces like British Columbia, Manitoba and others increases is unquestionable.
All of this is self evident to anybody following health care.
People lined up in Kingston desperately hoping to get a family doctor when a new clinic opened (image first put out by the CBC)
Except of course, the Ontario Government, and their Ministry of Health Bureaucrats. As far as they are concerned, now is actually the perfect time to attack family doctors. Because, you know, the way to improve burnout, morale and encourage them to take on new patients is to ambush people who are already under siege with overwhelming workloads.
Here’s what happened. About 6,000 family doctors in Ontario practice under what is called a Family Health Organization (FHO) model. Think of it as a base salary plus performance bonuses. As part of working in that model, the family doctors have to sign a contract agreeing to deliver a basket of services, including, a certain amount of after hours care.
Because we have so many rural areas in Ontario, where family doctors do a whole bunch of other work (emergency department, hospital on call, palliative care, long term care on call and more), there is a provision in the contract that says if you have X number of family doctors doing this kind of work already, then the amount of after hours care you provide as a FHO can be reduced. There’s a somewhat complicated formula but that doesn’t really matter – it’s the principle that counts. Essentially, if you are already doing after hours work – then you are not asked to do more after hours work.
Unless of course you are a Ministry of Health bureaucrat, taking the guidance of your bellicose negotiations team that said there was “no concern” about a shortage of family physicians. This allows you licence to use a stick against family physicians.
Dr. Jeff Tyberg, MOH Negotiations TeamDr. David Price, MOH Negotiations TeamDr. Darren Cargill, MOH Negotiations Team
Then, you send letters to 75 FHOs telling them they are not meeting the terms of their contract, based on made up metrics. The letters (I’ve seen a few of them) all allege that the doctors in the FHOs are not living up to the terms of their contract.
Let’s be 100% clear on this. If a physician signs a contract as part of a FHO, they should hold up their end of the bargain. You should read the contract, go in with your eyes open, and make sure you are capable of meeting all of the terms that you agreed to.
BUT.
It appears what the Ministry is arbitrarily and unilaterally determining how to decide if a physician is meeting the terms. For example, one FHO letter I saw suggested that that FHO was not performing as well as its “peers” and was therefore targeted. Two things though. First the Ministry unilaterally decided who the peers were. Second, performing up to the standards of your peers was not part of the original contract.
Another letter I saw alleged that the doctors who do call for their hospital or their nursing home, don’t qualify because……they don’t bill enough for going into the hospital. The ministry unilaterally decided that in order to claim after hours work, you couldn’t just be on call, but you had to keep going into the hospital when on call, a certain number of times (this number was never up for discussion before).
I’ll use myself as an example. Last Wednesday I was on call for my hospital. I got three calls (one at 4:00 am!) and managed all the patients over the phones. I DID perform the task I agreed to (being on call). But the bungling bureaucrats won’t acknowledge that. They want me go to the hospital (even if I can handle it over the phone) and then bill OHIP for the service (which would drive UP the cost!!) to be recognized – a decision they seemingly made on their own, without consultation.
My two loyal fans and one non-fan regular reader know that I’ve long maintained that Star Trek is a far better franchise than Star Wars. But in this case, I will concede the Ministry’s actions are most appropriately compared to this fellow:
Normally when a government changes the terms of an agreement unilaterally, one would expect the Ontario Medical Association to step in and advocate for their members. However, the response from the OMA, in a letter sent to all its members was, frankly, pathetic. The letter basically told doctors to “notify the Ministry” about the circumstances around your group. Try to reason with Darth Vader as it was. No dedicated email or legal team staff member either. Just contact the general help email.
I guess specialists who had expressed concerns on Social Media about too many family doctors on the OMA Board have nothing to worry about. Clearly the OMA, between allowing the across the board increases to the arbitration award this year and not dedicating resources to tackle this issue cares nothing about family medicine. (They talk a great game on social media, but it’s the actions that count).
I imagine the issue will eventually sort itself out after many rancorous meetings and back and forth – all of which will take up physicians time and prevent them from doing minor and inconsequential things like, say, seeing patients. The Ministry will continue to claim that we have more family doctors than ever before – but let’s face it, if they keep behaving like this, those doctors won’t practice comprehensive care medicine. It just seems so ridiculous, and indicative of a Ministry that truly doesn’t understand or value family medicine.
And that should frighten the general public more than the Death Star ever did. (Drat, made ANOTHER Star Wars reference).
The original Death Star from Stars Wars, Episode IV: A New Hope
Disclaimer: The information below is based on what a non-lawyer (i.e. me) was able to sort out after reading the OMA and Ministry’s 2024-2028 Procedural Agreement, the OMA Legal Counsel’s summary of the award, and attending the OMA Zoom session on the award. This may not be accurate (and I will correct the blog if more relevant information becomes available). I encourage all OMA members to contact the OMA directly with specific questions (info@oma.org) and not rely on this blog as your sole source of information.
OMA Negotiations Counsel Howard GoldblattOMA Negotiations Counsel Steve Barrett
The Numbers
First, let’s again review the numbers (approximated for simplicity).
Physician Services Budget, fiscal year ending March 2024: $16 Billion +
Arbitration Award: 9.95% – approximately $1.6 billion
OMA/MOH agreement on split of funds: 70% ($1.12 Billion) to fee increases and 30 %( $480 million) to targeted programs.
Previous contract (no guarantee this will repeat): 25% of the fee increases ($280 million) would go to across the board (ATB) fee increases for entire profession. The remainder ($840 million) would be distributed on the basis of relativity (giving more of a raise to low earning specialties and less to higher earning specialties). IF this pattern repeats, this equals a 1.75% increase for everyone. Then each specialty would get assigned an additional percentage (let’s say X) based on relativity. Ergo everyone should get 1.75% + X, where X varies from zero (for high billers) to higher (for lower billers).
The Implementation
According to the OMA webinar, the OMA and Ministry have yet to agree how to distribute the award. Mediation starts early October and all of this might wind up in Arbitration in March of 2025. My sense from watching the webinar is they are not close on an agreement.
So what happens to the money for this year? We are all supposed to get a raise now right? Well, that’s when the procedural agreement takes effect. It states (sorry for the legalese):
The Year 1 price increase will be implemented as follows: a. The entire price increase under the Year 1 2024-28 PSA will be implemented prospectively as an across-the-board increase to the fee-for-service payments identified in paragraph 1a above, with a target date of the RA in the month 90 days following the issuance of the arbitration decision, and will flow through to non-fee-for-service payments as soon as practicable. b. A lump sum payment equal to the entire increase awarded for Year 1 for the earlier period from April 1, 2024 through to the implementation date under paragraph 12(a), will be paid as soon as practicable following the arbitration award with a target date of October 2024. c. To the extent practicable, the permanent year 1 non-targeted price increases will be implemented at the same time as the April 1, 2023, price increases under Year 3 of the of the 2021-24 PSA i.e. April 1, 2025, and in any event no later than October 1, 2025. These increases will be calculated on a base of 2023-2024 expenditures …… The distribution as between across the board increases and relativity increases will be determined in such manner as the parties agree or, failing agreement, as the board of arbitration awards….
OMA staff confirmed at the webinar that this is in fact what will happen. They even had a complex schedule of prospective payments/lump sum payments/retroactive payments and so on that left me, frankly in need of high doses of Zofran.
To try and simplify things, let’s look at how this will affect two doctors.
Meet Drs. Alpine and Valley
Dr. Alpine and Dr. Valley both completed four years of an undergraduate degree. They then completed four years of medical school, and each did a five year residency in the field of their choosing. Dr. Alpine was always someone who liked to “do stuff”. He wound up in a speciality that does a lot of procedures and as technology has improved, has been able to treat more patients in a day than his specialty could 20 years ago.
Dr. AlpineDr. Valley
Dr. Valley, who is no less smart, really enjoys patient interaction. She chose a specialty that requires more intensive time with patients, and as such, is not able to see more people in a day than someone in her field could 20 years ago.
With our aging population and increasingly complex health care needs – both Dr. Alpine and Dr. Valley are swamped and have long waiting lists.
Dr. Alpine, was able to bill OHIP $1 million for fiscal year ending March 2024. This represents his gross income, and to be fair, his office has a lot of leased medical equipment, along with staff that he has to pay for out of that $1 million. Dr. Valley billed OHIP $350 thousand for fiscal year ending March 2024. She too has staff and other overhead expenses, but not as much equipment.
What happens to Dr. Alpine and Dr. Valley under the procedural agreement? While the schedule for payments for the award is a convoluted mess, the reality is that for the fiscal year ending March 2025 – Dr. Alpine will gross $1.1 million, and Dr. Valley will gross $385,000.
Now the OMA states that the goal is to have new permanent fees in place based on relativity and targeted funding for April 1, 2025. The ONLY way this could happen is if the government negotiations team completely capitulates its positions in the next couple of weeks. Seriously people, the schedule shows that if there is no agreement this thing goes to Arbitration in early March 2025. IF that happens, it’s part and parcel of Arbitration for the 2-4 years of the contract. So the Arbitrator probably won’t even make a ruling until September 2025. Then another six months to re program the ancient OHIP computers and while the fees may be retroactive to April 1, 2025, you likely won’t see the money until Spring 2026.
Let’s assume that the arbitrator follows the precedent set where 1/4 of the increase ( $280 million) should indeed be ATB, and then distributes the rest based on relativity. And let’s assume that Dr. Alpine’s speciality was assigned an X of 0% and Dr. Valley got an X of 18.25%. Therefore Dr. Alpine for the fiscal year ending March 2026 will gross $1.0175 million – a reduction of $82,500 dollars from the year before. While Dr. Valley will get bumped to $420,000.
No matter how often the OMA reminds people that the increase for the first year is one time only, and NOT a permanent increase, the reality is that many members will have budgeted around their increase, and Dr. Alpine will, be very miffed at a $82,500 reduction in income for doing the same work.
But it’s not all that great for Dr. Valley either. She will have missed one year of a substantial increase that should have gone to her earlier. Not only that, but her offices cost pressures and admin workload have been skyrocketing. She needs the stability a relativity based formula provides right now, not in March of 2026.
Because of the delay in stabilizing her practice, she actually chose to leave her practice and do a different kind of medicine. Her patients now have to go back on a waiting list, and who knows when they can find someone to take over their care.
I understand why this procedural agreement was put in place. It was to ensure that doctors got a much need cash injection sooner rather than later. But unfortunately there are unintended consequences of this and those are coming to fruition. Specialists like Dr. Valley who need the relativity increases right now will not be able to hold out and may leave their practices. Dr. Alpine will be understandably miffed at the yoyoing of his income.
And all of this uncertainty will do nothing to help the health care system.
On Sep 12, Ontario Medical Association (OMA) Board Chair Dr. Cathy Faulds announced that the Kaplan Board of Arbitration awarded Ontario’s doctors 9.95% for the first year of their Physicians Services Agreement (PSA). Sounds straightforward right? Nope – it’s actually ridiculously complicated.
OMA Board Chair Dr. Cathy FauldsWilliam Kaplan, Kaplan Board of Arbitration
I’ve looked at the award. I may have some of this wrong (copious documents found on the OMA website induced catatonia, hypersomnolence and cluster headaches). But this is my take.
A simplified (I have a small brain) set of numbers first:
Total award: 10%, approx value $1.6 billion dollars
Amount for general feel increases: 7% or $1.12 billion dollars
Amount for “targeted funding”: 3% or $480 million dollars.
In the past the OMA and Ministry agreed 1/4 of the raises would be across the board, the rest done with “relativity in mind”. IF we do that again then $280 million (1/4 of $1.12 billion) will be in across the board increases. Every specialty would get a 1.75% raise. The rest of the money ( $840 million) would be for raises based on relativity. So all specialties would get 1.75% + X as a raise. The “X” would vary. It would be more for low income specialties, and the X would be lower or even zero, for the high income specialties.
The Good. There’s a raise. The MOH Team stated that Bill 124 should not impact the deal. The arbitrator disagreed and felt that we were unfairly treated because of Bill 124 stating:
“Bill 124 directly impacted the bargaining even though physician compensation was not subject to its terms.”
Hence, the MOH Team completely lost their argument that there should be no redress, and there was a 6.95% redress given.
There was a recognition that family practice is in crisis. In his ruling the Arbitrator said:
“We accept on the evidence that there is a physician shortage. Somewhere between 1.35 million and 2.3 million people in the province are not attached to a family doctor. These are real numbers. The Ministry’s own documents – which we ordered disclosed–demonstrate that there is a problem to address.”
The arbitrator had to order the Ministry to disclose this?? Jeez. Additionally, the Arbitrator noted:
“Clearly, more family doctors are needed as are more doctors practising comprehensive longitudinal medicine…..it is obvious that the citizenry is ageing – the Government acknowledges this brings with it increased complexity…”
Contrast this with the Ministry’s absolutely laughable position that there is “no concern” about a shortage of doctors. This is frankly a warning shot, and a welcome one, to the MOH’s negotiations team to not say such stupid things again, and to change their position in future rounds of negotiations.
Dr. David Price, member of the Ministry’s negotiations teamDr. Darren Cargill, member of the Ministry’s negotiations teamBob Bass, member of the Ministry’s Negotiations Team
In another shot to the now obviously inept MOH Negotiations Team, the Arbitrator agreed that admin burden also needed to be addressed with, you know, money. He stated:
“We have reached the conclusion that targeted increases – not necessarily baked in – should be allocated to the reduction and redeployment of administrative work that can best be performed by others or through digital or other measures.”
Finally, It was quick. OMA Board Chair Cathy Faulds had told us not to expect an award until the end of September. Who knows why Kaplan put the award out so quickly.
The Bad.
This will not be enough. The OMA asked for a 22.9% increase. They got less than half of that. This is not really the big win the OMA is portraying it as.
A 10% increase in gross billings for family medicine will not be enough to stop the haemorrhaging of doctors from comprehensive family practice. The “X” for family medicine (see above) needs to be high, and much of the targeted funding needs to go to family medicine too.
And, while it’s true that the Arbitrator recognized there was a crisis in family medicine, the award given did not really do anything in and of itself to stabilize family medicine. It’s true that was not part of the scope of the arbitrator for this round (this round was for a fee increase). The fact that some practical guidance in how to resuscitate family medicine is missing is still bad for all Ontarians.
The Ugly
The implementation of this award is going to be a nightmare. As I write this, there is no indication that the MOH and OMA have agreed on how to divide up the $1.12 billion in general fee increases based on relativity. In fact, indications are that the MOH will continue to fight the methodology, meaning it could be a very long time before fee increases for specialties are set.
Worse, the OMA and MOH have not been able to agree on how to distribute the $480 million in targeted funds. Which means….more mediation and arbitration. I continue to concede that the OMA states arbitration and mediation will be done by mid- March 2025. I continue to not hold my breath.
Even uglier is that one solution being proposed would be to give “everyone” a 9.95% increase right now, until the relativity and targeted funding is sorted out. But that would mean that some of the higher paid specialties would see a 9.95% for a bit, only to have a relative cut once the final fees are sorted out (also to be arbitrated by March 3-7, 2025). No matter how you message this to warn people – this will cause problems when people see a decrease in income after a rise.
All of which means that the retroactive pay for this year may not come for over a year. If you are a physician who has some decisions to make (eg do you renew the lease on your office at the higher rates the landlord is demanding) – you are going to be awash in uncertainty.
The ugliest part of all of course, is that a bunch of lawyers are going to get really rich as their billable hours go through the roof during this process.
There is a better way.
The government’s main concern should be about expenditures. That decision has now been made for them. The PSB will go up by $1.6 billion. That money will have to be paid one way or another.
The government can now, especially after being told off by the Arbitrator back off from their polarizing and obstructionist path, accept the OMA proposals for implementing the award. They cover what the government states it wanted (pay lower paid specialist more of an increase than higher paid ones). They also covers issues around admin burden which the Arbitrator acknowledged exist, and the shortage of family physicians (which the arbitrator also acknowledged).
The total amount spent by the government is going to be $1.6 billion regardless. Getting rapid agreement on the distribution of those funds will decrease the uncertainty about how much goes where and will shorten the time it takes doctors to get paid, which will stabilize the health care system.
Then, for the love of Allah/God/Yahweh/Great Universal Consciousness – the government now needs to realize that you can’t fix health care without working co-operatively with your doctors. Go look at other provinces. Copy them and get a fair deal for years 2-4 of this agreement.
Or the government can continue to obstruct, obfuscate, delay and impede any real progress towards working together with more protracted, internecine mediation and arbitration. The ball is in their court.