Dear OMA Board Member,
Just me again. The grumpy, aged quack with a history of being a bit of a thistle in your obliques. Well intentioned I assure you (although I’m told some may not see it that way).
Negotiations with the provincial government on a Physicians Services Agreement (PSA) continue and mediation began on February 20th. That’s all great and part of the process. However, things HAVE CHANGED a lot since the last time I wrote to you and urged you to set a strong mandate.
I am asking you to revisit the negotiations mandate at this time, in light of three new key pieces of information that are very relevant to Ontario doctors.
To recap – the negotiations mandate is the bare minimum ask that the Negotiations Task Force (NTF) can accept on behalf of the Board. If the government makes an offer that meets or exceeds that – well, then they accept it on behalf of the Board and the Board is compelled to endorse it. The mandate is, quite correctly, confidential (you can’t let the other side know your bare minimum ask any more than they would let you know their mandate). But it’s up to the Board to determine if the mandate is enough (not the NTF).
Now to be clear, I’m not saying you should revise it, just revisit it. Perhaps the mandate is already sufficiently strong. That would be great. But things are different now.
The first reason to revisit the mandate:
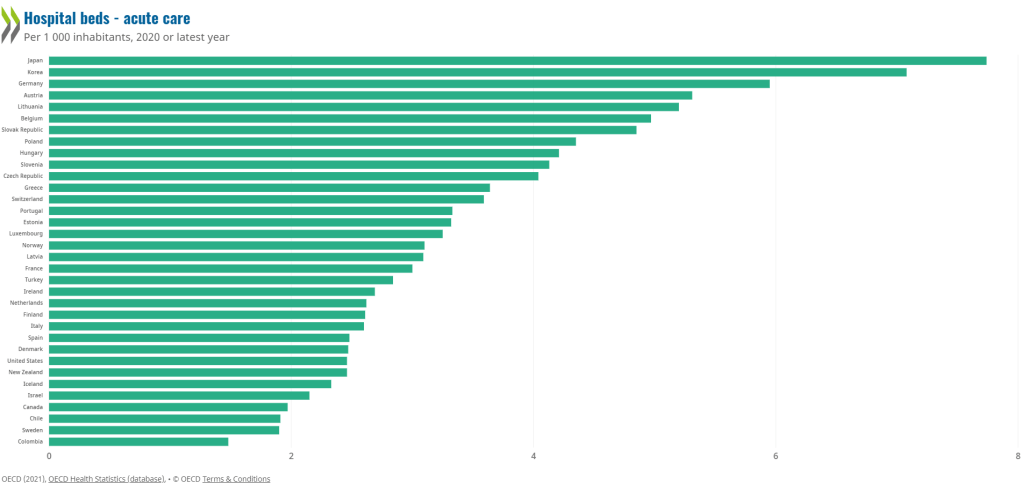
Other provinces have surpassed Ontario physicians in terms of income. BC and Saskatchewan have significant deals to stabilize the physician work force. Manitoba’s deal with physicians appears to be the best of the bunch. Manitoba has not only a well deserved increase for all physicians, but significant steps towards gender pay equity.
As an aside, while I applaud the fact that DoctorsManitoba made steps towards gender pay equity, I’m forced to wonder what happened to Ontario? When I was on the OMA Board we were proud of the fact that although it was too late, we were the first PTMA to report on the issues around gender pay equity. We proved that the pay gap was not because “women work less hard”. What happened ?
Also, to be clear I want to acknowledge that the negotiations counsel (Messrs Goldblatt and Barrett) are very well aware of any topic that could affect negotiations. I remember Darren Cargill, who at the time was on our NTF, told me “they read everything.”


Therefore, I know they read the Manitoba Schedule of Benefits which is available online and reported back to you. I’m sure you are fully aware of the retention bonuses in that deal. I’m sure you know about the significant changes that decrease the gender pay gap. I’m sure you know about the fact that Manitoba pays physicians for Admin time. And that their capitation model has no negation (although a lower base rate). And that they have an age premium. A pelvic exam premium (gender equity again). And that they allow extra payments for dealing with more than one problem at a visit. I have absolutely no doubt that our negotiations counsel has fully and thoroughly advised you of this, along with the benefits of the deals in BC and Saskatchewan.
The second reason to revisit the mandate:
The crisis in family medicine is spiralling out of control, faster than I thought possible. Not only is it badly affecting patient care, but the health, well being and morale of physicians is sinking like a stone. Last September, I never dreamed that I, along with Drs. Alam and Mathew, would write a letter to Family Practice residents telling them to stay away from comprehensive family medicine in Ontario. I never dreamed that there would be story after story after story of individual family physicians openly talking about how they were burning out. This situation has gone form bad to desperate frighteningly quickly.
The third reason to revisit the mandate:
Bill 124, the piece of legislation that limited increases to the public sector, was used to promote a low ball PSA to us the last time. You even, admittedly and embarrassingly, convinced a guy who should have known better. It’s ruled unconstitutional and the government will not appeal this. In fact they will repeal the Bill entirely. In light of that, many other public sector workers will be asking for catch up pay.
So it really is time for you to re-visit the negotiations mandate. Just double check to make sure it’s as strong as it should be given the above factors. Make sure it takes into account that the the BC deal has attracted over 700 physicians to comprehensive family practice. Make sure it recognizes that Manitoba will likely be showing a net growth in physicians shortly, and can reasonably attract physicians from out of their province. If you have to revise the mandate upwards after looking at it, then do so.
NB – IF the NTF were to push back if you do revise the mandate upwards, then make sure you hold your ground. Remember, YOU are the Board and YOU give direction to ALL committees and task forces, including the NTF. I’ll be careful how I say this so as not to divulge Board confidentiality, but the NTF in my day did have a proposal on one particular issue (not the whole PSA) that they told us to approve and our Board pushed back and said no. We had to listen to some (quite eloquent) speeches about how hard they worked and this undermined their work and so on and so forth – but after that they went back and kept negotiating as directed. Don’t do any less this time.
These negotiations are likely to make or break the profession for decades to come. They are that important. You owe it to your members to take another look at the mandate.
Yours truly,
An Old Country Doctor.