Recently Maria DiDanieli, a system navigator with the Burlington Family Health Team who holds a Masters in Medical Bioethics, wrote an article criticizing myself, Dr. Silvy Mathew and Dr. Nadia Alam for recommending family medicine residents NOT start a comprehensive care family practices at this time. Dr. Mark Dermer responded so eloquently to that, that I asked his permission to reproduce his response as a guest blogger, and he kindly agreed.

As a recently retired family physician, I am troubled by the fact that you (Maria DiDanieli) have mistaken the fact that you work adjacent to family doctors as sufficient to understand what they face. Worse, your assessment of Drs. Alam, Gandhi and Mathew is unjust.
But that’s not why I am commenting. Instead, I am coming at this as someone with some experience in medical ethics, both as a long-time member of community and teaching hospital ethics committees, and as a teacher of medical ethics to family medicine residents.
To put it simply: Your ethical analysis of my colleagues publishing the opinion piece in question is both facile and flawed.
I crafted an ABCDEF mnemonic to help residents remember six fundamental principles of medical ethics:
A – the right to Autonomy in decision-making
B – the moral duty of physicians to be adhere to Beneficence when caring for patients
C – the obligation to safeguard patient Confidentiality
D – the patient’s right to receive Disclosure of all information pertaining
E – Equity in dividing finite resources among patient populations
F – First, do no harm (nonmaleficence)
We then apply these principles to a given situation, understanding that the principles might conflict with one another. It is very rare that a single principle can be used to judge a given question. We also must accept that there are almost never absolute rights and wrongs, just better and worse answers.
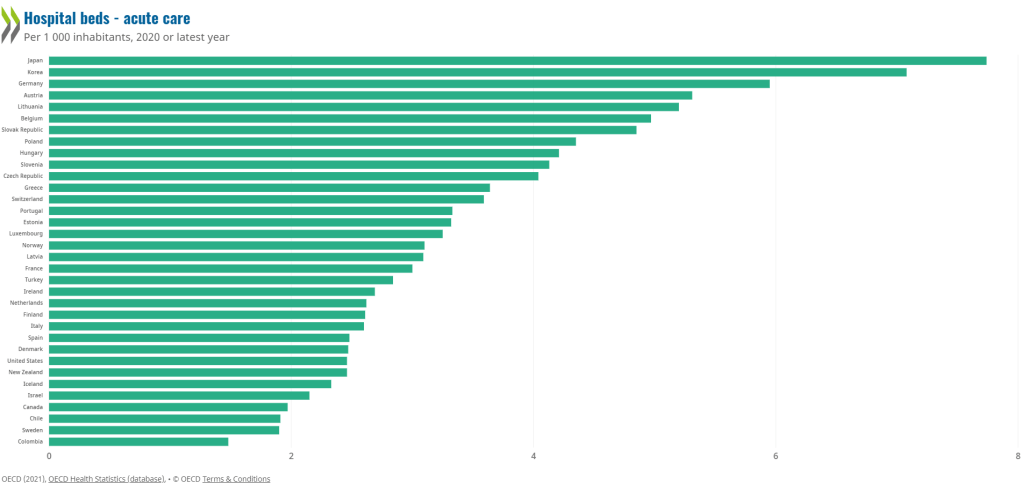
I am confident that we can agree that the current primary care crisis is first and foremost a violation of equity: present circumstances have divided the people who want a family doctor into those who have one and those who don’t. I also expect that you are aware of the evidence that demonstrates that patient outcomes are better when people have an ongoing relationship with a family doctor.
But you make the elementary mistake of applying a single ethical principle, nonmaleficence, to the matter at hand. Furthermore, you seem unaware that physicians graduating from family medicine programs have been entirely consumed with their training over the previous 5-6 years, nor aware that the medical education system has largely withheld what graduating residents will face as they enter practice. In that light, the letter is a long overdue disclosure that brings transparency to the current state of family medicine.
That’s right, physicians have the right to disclosure too. We also have rights as people to autonomy, confidentiality and equity. Yet when it comes to our work, we are forced to accept legislated pay and work conditions from a monopoly payer, the government. And the government uses the fact that physicians are independent contractors to justify the fact that we are not entitled to the same cost-of-living increases paid to other health or educational professionals.
Finally, I think you fail to recognize that in family medicine, we face unusual challenges to persistently align with all the principles of medical ethics, which work best when applied to “cases” (a single patient at a single moment in time). In contrast, family physicians’ work is longitudinal and includes significant responsibility to populations of patients as well as to individuals. That means that we accept short-term harm when we do things like stick vaccination needles in people’s arms or wean them from opioids, understanding that we are looking to provide a net benefit in the medium to long term.
To my mind, that is precisely what Drs. Alam, Gandhi and Mathew have done. In other words, they are acting very ethically. For while the short-term consequences of their disclosure may accelerate the intensification of the immediate crisis, the sooner the crisis provokes action the sooner we start climbing out of this horrendous hole.