Disclaimer: I’ve looked through the OMA page on the FHO+ model and interpreted the data as best I can, BUT, this information should NOT be used by others for their own financial planning – they should review the data for themselves. Additionally, because this is a complex model – if the OMA’s Negotiations Task Force feels there are mistakes – I would be happy to correct those.
Last week, the OMA announced that they and the Ontario government had developed an enhanced model for paying family physicians. In Ontario, the most popular model for paying family physicians is something called the Family Health Organization (FHO). More physicians would choose it, but in typical unthinking and regressive fashion, the bureaucrats at the MOH convinced the government to limit entry into that model in the 2010s – because you know, why would you want people going into family medicine to have their preferred payment model? What were they going to do? Stop working as family doctors? Sigh…..
The OMA website states the new FHO+ is the “Future of Family Medicine” and talks glowingly about how this will “bring back the joy of family medicine, and build a foundation to support recruitment and retention”.
It’s always tough to break things down with a new model, and there are a lot of variables and enhancements to review. I encourage all family physicians to watch my friend Dr. Adam Stewart’s set of truly excellent videos on this new model.
For my part, I consider myself to have a medium sized practice. I therefore looked at Dr. “B” on the OMA’s web page to come up with my thoughts. (Note to OMA – come up with some better names for the doctors!)
- How much of an increase in income am I going to get?
According to the OMA site, I should expect an increase of 13% of my gross income. But it’s not clarified what the baseline for that increase is? Is it this year’s income? Last year’s? So I emailed the OMA and was given this answer:
“The base rate the parties agreed to use in our costing was FY2023/24, keeping in mind the last permanent increases were on April 1, 2023, the recent years 2.8%, 9.95% and the monthly relativity for FY2024/25 are all temporary and will end on April 1, 2026.”
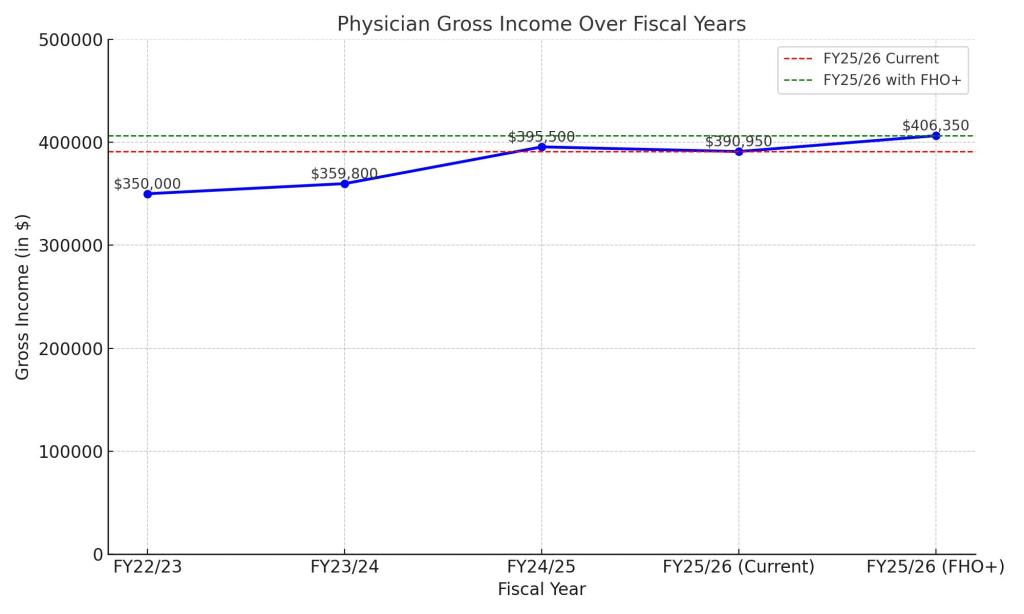
Alright, some more math (my apologies). Let’s use fiscal year 22/23 to start. Let’s assume I grossed $X in that year. For FY 23/24 – that was the last year of the previous PSA and we got a 2.8% increase in fees. So I grossed $1.028X that year. FY24/25 was year I of the current PSA and we were awarded 9.95% by the Arbitrator (compounded to the 2.8%). Because there was no agreement on how to divide it up, it was distributed equally among all docs. So I grossed $1.13X.
Still with me? This year, FY 25/26, by mutual agreement, there was a relativity based increase from the original FY 22/23. FHO docs like me got 11.7% so this year, for now, I will be grossing $1.117X. This is down from last year but may change based on whatever happens in Arbitration.
Based on the OMAs reply, if FY 23/24 is the base year they used in their calculations (when I made $1.028X) then and increase of 13% on that will translate to $1.161X. In essence, if FHO+ goes through, it will mean a 4.4% increase for me next year, compared to this year (1.161-1.117) and a mere 3% more than last fiscal year. Better than nothing? Sure. Is it the major dollar influx needed to save family medicine? I think you know the answer to that.
2. How will rural medicine fare?
One of the things that strikes me about this model is that effectively, rural medicine will not do as well. Now, in fairness, there are attachment bonuses for taking on new patients, and those bonuses are higher in rural areas. So there is that. But my understanding is that rural doctors are working overtime anyway and not really able to take more patients right now.
But what should be noted is that in the OMA calculations, the assumption has been made that doctors are getting at least some access bonus currently. So let’s look at Dr. Rustic and Dr. Metro, a rural and urban doc.

Let’s assume they also fall into category “B” as per the OMAs example. It is well known that urban doctors, despite how hard they work, have challenges getting the access bonus. Dr. Metro currently gets an access bonus of $0 because there are five walk in clinics with 15 minutes of her office. This is despite her group working after hours care. Dr. Rustic on the other hand, gets $25K in access bonus, mostly because his group is the only game in town.
With FHO+ the access bonus gone and repurposed to pay for other items (and that is a very good thing as my friend Dr. Mark Linder pointed out) in effect, Dr. Metro’s raise will be $25k MORE than Dr. Rustic’s. I don’t begrudge Dr. Metro the income, she deserves it. But in order to recruit in rural areas, we’re going to have to find a way to bump Dr. Rustic’s income more.
3. What exactly will the Accountability Metric be?
This is of course, the great unknown. These metrics are often presented as “reasonable” and then governments always find a way to make them unreasonable. We won’t know the answer to that until after Arbitration.
Final Thoughts
At the end of the day, I think family doctors as a whole need to realize that FFS family medicine has gone the way of the Dodo bird (I know this will upset some FFS purists). The government also seems to recognize this and as part of the agreement is increasing the number of FHO+ positions.

Despite some of the concerns above, I do think that FHOs should migrate to the new model. It is slightly more money, and I do wonder if by tweaking your practice more – the amount can go up. For example, I have about 200 patients whom I have not rostered because of outside use issues – I would now roster them – and this would increase my income even more. So I suspect there is potential to make more than a 4.4% increase if you manage your roster well. Looking at increased shadow billing rates also offers some potential for more growth.
However, saving family medicine requires a multi-pronged approach that requires a single, unified health information system, family practice teams with physicians clearly placed as the leaders of the teams (with funding for leadership roles) and much more than a 4.4% increase in income. So take the money for now, but don’t in anyway shape or form believe that this in and of itself will fix family medicine.