As provinces across Canada begin to lift restrictions from the Covid pandemic, there is a plethora of opinions raging about this. Some physicians feel the restrictions are being lifted too slowly. Others feel that it is just right. In Ontario at least, the most outspoken group are the physicians who demand ongoing restrictions. They have taken to using #Covidisnotover on Twitter.
Obviously, when dealing with a once in a century pandemic that has truly decimated patients and health care workers alike, there are still going to be unknowns going forward. But personally speaking, I think we have to realize a couple of things. First, Covid is not over. Second, and most importantly, it never will be.
Is the flu over? Is HIV over? Heck, are measles and RSV over? The answer to all of those is no. The viruses are still around, they are still infecting people and are mutating all the time (that’s why we need an annual flu shot).
There are always a certain amount of these viruses in the ecosystem. Why would Covid be any different? We are not going to completely eradicate Covid.
Given this – the question becomes, what do we do as a society?
One option, and certainly one that is promoted by the #covidisnotover types, is to continue ongoing restrictions, for much longer. Be it mask mandates, enforced vaccine passports, or continued limits on indoor capacity, the message from them seems to be to keep imposing restrictions for……well, I couldn’t really find consensus on an end date.
The most common argument for continuing restrictions (in Ontario anyway) is the continued positive case load. There are more positive cases than ever before, so why should we stop restrictions now?
Well, the short version is that while it is absolutely true that our case load is higher now than in, say October of 2020, many other factors have changed. In October of 2020, there were no vaccines. There were no oral medications that could help treat those who were infected. Guidance on the fact that Covid is airborne was still (shockingly) lacking.
In comparison, in March of 2022 over 90% of the adult population of Ontario has two covid vaccines, and are well on the way to their third. Evidence is clear that the vaccines are remarkably effective at preventing serious complications of Covid. There is now a strong emphasis on good ventilation as a way to reduce the Covid burden. The government is providing funding for Hepa filters in schools and child care settings. A protocol for rolling out the new oral medications exists, and, like all things, supply of the medications will increase with time.
So to compare just case numbers from October 2020 to March 2022, quite frankly is just comparing apples to oranges. We need to take all these other factors into account.
The other common argument is essentially “Look at Denmark!“. Pro restriction types point to the fact that Denmark lifted all Covid restrictions on February 1st, 2022, and now seems to have an exploding number of cases and mortality. Graphs like the one below are designed to shock people into thinking there is a catastrophe in Denmark:
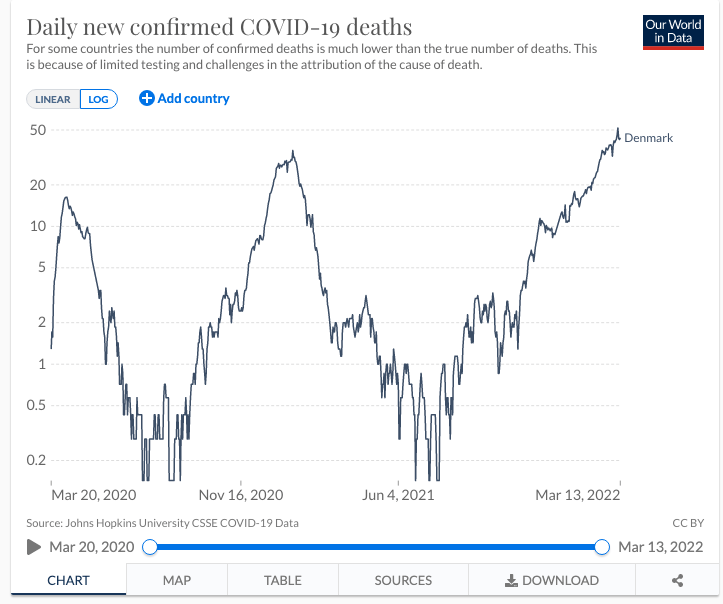
But the graph doesn’t tell the whole story, and in fact a much more nuanced approach requiring a deep dive into the data is needed. I was going to try but I can’t do a better job of it than Michael Petersen did in his twitter thread:
The short version is that because so many people have Covid now, we need to do a better job of determining who died because of a covid infection (usually a covid pneumonia) vs who died of other causes, but incidentally happened to have Covid at the same time. A better graph showing the Denmark situation (taken from Petersen’s thread) taking this into account is here:
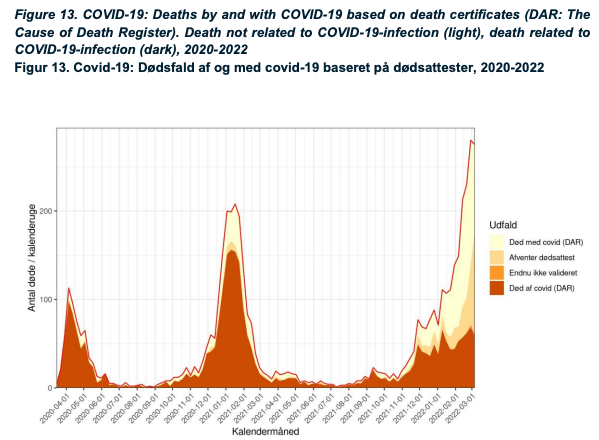
Before people start jumping all over this, let me also point out that I am acutely aware that there is a significant spike in deaths in Denmark recently, even if not specifically caused by Covid. We clearly need to do a deeper dive into why there were excess deaths. But part of that deeper dive must include whether deaths were caused by the restrictions themselves (delayed care, depression and mental health issues leading to people just giving up etc). In essence, is the cure (restrictions) causing more harm than the disease (Covid)?
Look, lockdowns and restrictions were initially necessary. There is good evidence that they helped to blunt the course of Covid. But there is also evidence that they have harmed society as well. The economic impacts with record government deficits that will tax our great grand children are well known. However, there are also other health care impacts.
In Ontario, we have a back log of 20 million health care services, leaving many patients feeling forgotten. There are consequences to delayed care and I have seen that in my own practice, and expect to see much more in the coming year. Yes, those consequences sadly will include deaths.
All of this is before we even consider the collateral damage done to mental health especially in our pediatric population. As Dr. Jetelina points out in her excellent sub stack, there has been a world wide increase in paediatric mental health issues. A 24-31% rise in children presenting with mental health issues and a shocking 69-133% (depending on age group) increase in children presenting with suicidal thoughts to Emergency Departments.
What does all this mean?
My personal feeling is that while we cannot ignore Covid (it’s a bad disease) and we need to continue to encourage vaccinations (they work), we need to start looking at the health care system as a whole. Should we mask in high risk areas? Sure. But should we continue to isolate people socially and restrict interactions in a lower risk population, when that clearly causes other harms? I would argue no.
We have been making decisions for a long time based on Covid numbers alone. There are other illnesses and disease that are out there, many of which have been worsened by the restrictions Covid has forced on us. We need to start basing our health care decisions on what’s best for overall population health, not just Covid.