The following blog was written by Dr. Darren Cargill (pictured inset) and originally appeared in the Medical Post in a modified form and it’s full form on his substack. It’s a great message for medical students who didn’t match on CaRMS day, and is being re-printed here with Dr. Cargill’s permission (and my thanks) so that it is more widely available in an un-gated site.
J.J. McCarthy and the UnMatchable
“Those Who Stay Will Be Champions”
On November 14, 2020, Michigan was blown out by Big Ten rival Wisconsin by a score of 49-11, dropping the Wolverines to 1-3 in a pandemic-shortened season. Questions were swirling about if former Michigan quarterback Jim Harbaugh’s would remain as head coach at his alma mater. The Wolverines would finish a the season a disappointing 2-4.
On November 15, J.J. McCarthy sent out this tweet:

What does this have to do with health care in Canada?
I have previously written about my own failures and setbacks. From dropping out of University in 1994 (and 1995, just to be sure), to going unmatched through CaRMs in 2003.
Match Day 2024 is March 19th. I could have simply reposted my Substack from last year and moved on.
But Michigan’s 2023/24 run to the National Championship was calling me.
Anyone who knows Michigan football understands how it works. They run the ball down your throat. They tell you what they are going to do and then challenge you to stop them. Four yards and a cloud of dust. Big Ten Football.
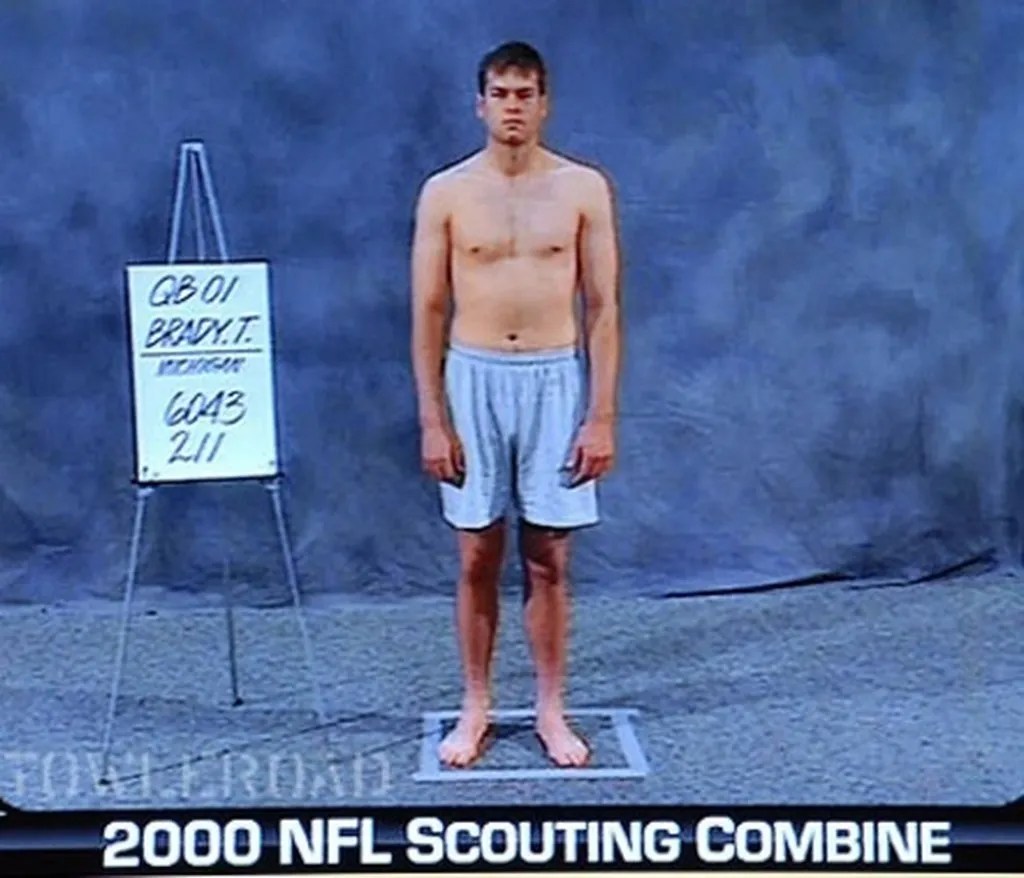
Former Michigan QB Tom Brady played with a chip on his shoulder his entire career. After winning a national championship at Michigan in 1997, Brady was drafted 199th in the 2000 NFL draft. He was not expected to be the GOAT, experts weren’t even sure he would make the team. Yet 10 Super Bowls later (and 7 rings), he is the undisputed greatest Quarterback of all-time (talk to me about Patrick Mahomes in 20 years).
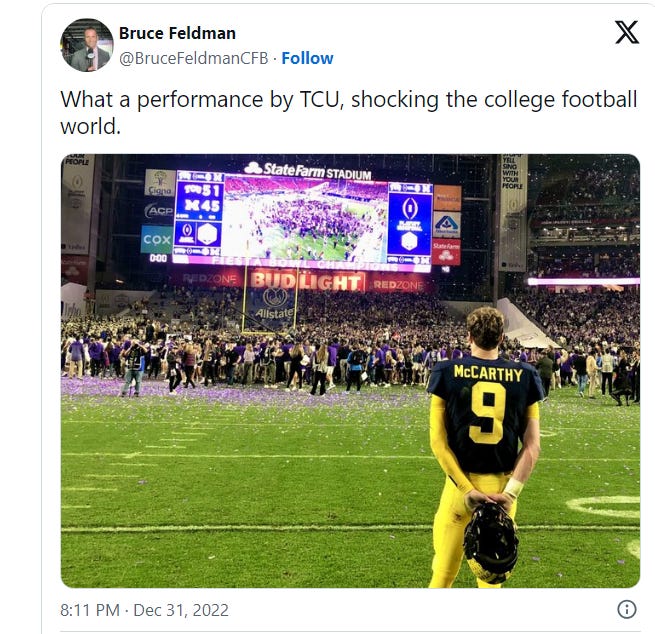
After Michigan’s loss to TCU in the College Playoff last year, McCarthy stood on the field and watched TCU celebrate.
As detailed by Sports Illustrated: “There’s perhaps no greater insight into an athlete’s psyche than seeing how they act following a crushing loss. Michigan quarterback J.J. McCarthy gave fans a small glimpse into his mindset after the Wolverines’ devastating 51–45 defeat in Saturday’s Fiesta Bowl.
Playing in the College Football Playoff for the second straight year, Michigan (13-1) was unable to overcome a handful of missed opportunities and came up just short in the national semifinal against the Horned Frogs.”
I see a lot of Brady in McCarthy. Quiet confidence. A leader of men. Resolve in defeat.
Today, J.J. is QB1 for the 2024 College Football National Champion 15-0 Michigan Wolverines.

J.J. enters the 2024 NFL draft this spring. A lot of people (usually Buckeyes) question his ability. They call him a “game manager.” They doubt his arm strength.
Going unmatched in 2003 gave me some serious doubts about my abilities. My skills.
Was it a mistake to go into medicine? Could I be happy in another field? Did I leave the stove on?
Today, I am the only physician in North America with Fellowship in the College of Family Physicians before Canada, Royal College of Physicians and Surgeons of Canada and the American Association of Hospice Palliative Medicine.
The NFL draft is much like the CaRMs match. It distills years of hard work and sacrifice into one binary answer: matched/unmatched.
To my fellow UnMatchable: Take 3 deep breaths…and have faith.
“Destiny is calling. Open up your eager eyes.”
#GoBluE

PS I rushed the field at Michigan Stadium for the first time this year when the Wolverines beat THE Ohio State Buckeyes (again). Destiny calls.

I then watched the Championship game with my friend Mark, who recruited me to Windsor. Destiny calls.