Dr. Ken Milne (pictured inset), an Emergency Room physician for almost twenty years and an associate professor of medicine at the Schulich School of Medicine and Dentistry (among many other things). He wrote an excellent X post recently, based on an interview with Dr. Ross Prager. He has graciously allowed me to republish here as a guest blog. I think the advice he gives is outstanding, and is a must read for all medical students (and frankly some of us older docs too).
For all the new medical students starting this fall there are 10 lessons they don’t teach in medical school (but should):
One – Patients don’t care how much you know, but how you make them feel.
Two – You’re remembered by your worst moments. When stress hits, your true self emerges…that is what people remember. Grace under pressure matters more than glory during routine.
Three – Stop trying to impress people with knowledge.
Four – Being keen is not a crime. Passion is a virtue, not a vice. Don’t hide your enthusiasm…it’s a sign you care.
Five – Medical School and Residency are long job interviews.
Six – Absence of evidence ≠ evidence of absence. Not everything is backed by RCTs (randomized control trials). That doesn’t mean it’s invalid. Clinical observation and physiologic rationale matter. As always, be skeptical of the lack of evidence, too.
Seven – Character is how you treat people who don’t supervise you.
Eight – Focus on diagnosis first, treatment second. Most medical harm arises from misdiagnosis, not mismanagement. Think ten times harder about “what’s going on” before “what should we do?”
Nine – Don’t postpone living until after residency.
Ten – Remember the spark. Recall your first patient: the awe, the uncertainty, the honour. When burnout creeps in, revisit that moment. Reconnect with your “why.” Medicine is not just about answers, it’s about presence. Our best tool is our humanity.
Educating the mind without educating the heart is no education at all. Aristotle quote
So, to all the new medical students…get ready for a great adventure. There will be times of joy and sorrow. If you are struggling at some point, remember, it is ok not to be ok. Reach out to friends, families, mentors or counsellors. Your attending physicians may look like they have it all together, but we have all struggled at some point & needed help. You can read my story here. This is another good episode for students and residents to listen to.
Old Country Doctor’s thoughts: On a personal note I want to welcome all of the new entrants to medical school this year. You will have experience incredible joys during your medical journey, and you will have your share of sorrow. To experience those sorrows is not a failure, it is life. But always remember, by being accepted to medical school, you have already proven you’ve go what it takes to succeed and to help others. You yourself may need help sometimes (we all do) but you’ve got this.
“Medicine cures disease, but only doctors can cure patients” – Carl Jung.
Dr. Mark Dermer (pictured inset) , a recently retired family physician guest blogs for me today. He posted his thoughts about the arbitration process and how it can potentially affect family medicine on a private facebook group. I thought his post was excellent and I’m honoured that he has agreed to allow me to republish his thoughts here, so more people can see it.
A common misconception about how the arbitration decision will be determined is that the arbitrator will choose either the entire OMA submission or the entire MOH submission as the PSA award for 2025-28. While some arbitrations work like that – salary arbitration does – that’s not the case in the OMA-MOH 2017 Binding Arbitration Framework (BAF). As stated in paragraph 18 of that document (in this group’s files section):
“Absent an agreement of the parties, the method of binding interest arbitration to be used shall not be final offer selection. In particular, unless the parties agree otherwise, the arbitration board may, on any issue or issues, select either party’s proposal, choose a middle ground, or issue any award that it determines is appropriate in the circumstances.”
In other words, the arbitration board will issue a decision that is built point-by-point, with quantitative decisions set anywhere on the continuum between the two parties submitted positions. And the choice for each point/issue will be made in the context of the entire Physician Services Agreement (PSA).
For family physicians, there are four points of dispute that await the final PSA arbitration decision:
1) Annual increases to the Physician Services Budget (PSB) in years 2, 3 and 4 (2025-26, 2026-27 and 2027-28) of the present 2024-28 PSA. Note that these overall increases will then be subject to relativity adjustments that are managed within the OMA.
– OMA submission: 3.75% in each of the three years for a total of 11.25%
– MOH submission: 2.25% year 2, 2% in years 3 and 4 for a total of 6.25%
The arbitration board will award a percentage amount for each of the three years that lies on the range between the two parties submitted figures guided by the information supporting their numbers (the OMA’s justifications for its figures in its submission look to my eyes to be considerably stronger).
2) Continuity of Care Accountability Measure with Financial Consequences – the methodology of the measure has been agreed by the parties. But the question of whether there will be financial consequences and if so, the trigger threshold and financial magnitude, have not.
– OMA submission: no financial consequence but if so, trigger threshold should occur only if continuity falls below 70% and penalty should be a 10% reduction in base rate
– MOH submission: Trigger threshold is falling below 80% continuity and penalty should be 20% reduction in base rate
The arbitration board must first decide whether there should be a financial consequence and if so, when it should be implemented. For example, it could say that physicians need several quarterly reports to allow them to adapt their practices before the financial penalties start. With respect to the threshold, the arbitration board will likely choose a figure in the 70-80% range, though it is free to choose outside that range and here to, it could make a setting that changes over the three remaining years of the agreement. Same goes with the size of the base rate penalty, which we can assume will be in the 10-20% range if a penalty forms part of the new PSA.
** Note – Continuity of Care and any penalty is assessed at the level of each individual physician’s practice, NOT at the level of the FHO.
3) Increase to FHG premium
– OMA submission: Increase from the current 10% to 20%
– MOH submission: No change
The arbitration board may choose to keep the FHG premium the same, or increase it by any amount it wishes. Including raising it by more than 20%.
4) $5 per patient visit overhead fee for community practices (up to 40 visits per day; excludes hospital, contract and FHO/FHO+ services)
– OMA submission: Newly proposed by OMA
– MOH: No response
The arbitration board will have to decide whether to introduce this fee at all and then at what dollar rate to set the fee. Note that this fee applies to community specialist practices as well as to non-FHO family medicine practices.
The bottom line:
There is a wide range of possible financial outcomes of the arbitration board award. That’s why trying to forecast how it will affect you, or plan adaptations, will likely not be a very good use of your time at the moment.
I also think that the past week has demonstrated, yet again, the OMA’s poor member communication skills: it was irresponsible of them to publish scenarios and calculators that neither acknowledge nor take into account the possible continuity of care financial penalties. My recommendation is to generally ignore their messages until the arbitration board issues its decision.
Disclaimer: I’ve looked through the OMA page on the FHO+ model and interpreted the data as best I can, BUT, this information should NOT be used by others for their own financial planning – they should review the data for themselves. Additionally, because this is a complex model – if the OMA’s Negotiations Task Force feels there are mistakes – I would be happy to correct those.
Last week, the OMA announced that they and the Ontario government had developed an enhanced model for paying family physicians. In Ontario, the most popular model for paying family physicians is something called the Family Health Organization (FHO). More physicians would choose it, but in typical unthinking and regressive fashion, the bureaucrats at the MOH convinced the government to limit entry into that model in the 2010s – because you know, why would you want people going into family medicine to have their preferred payment model? What were they going to do? Stop working as family doctors? Sigh…..
The OMA website states the new FHO+ is the “Future of Family Medicine” and talks glowingly about how this will “bring back the joy of family medicine, and build a foundation to support recruitment and retention”.
It’s always tough to break things down with a new model, and there are a lot of variables and enhancements to review. I encourage all family physicians to watch my friend Dr. Adam Stewart’s set of truly excellent videos on this new model.
For my part, I consider myself to have a medium sized practice. I therefore looked at Dr. “B” on the OMA’s web page to come up with my thoughts. (Note to OMA – come up with some better names for the doctors!)
How much of an increase in income am I going to get?
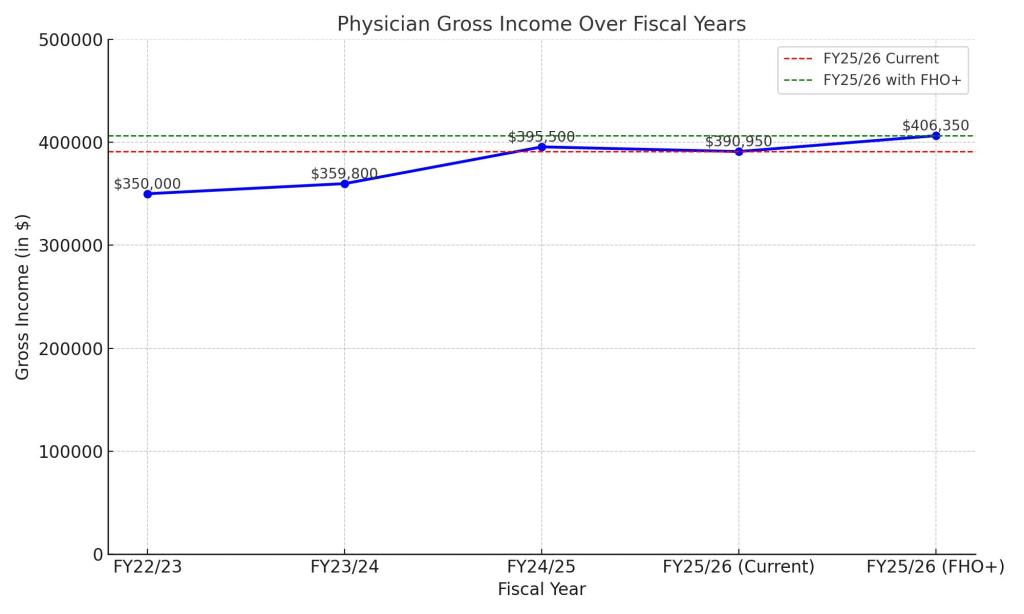
According to the OMA site, I should expect an increase of 13% of my gross income. But it’s not clarified what the baseline for that increase is? Is it this year’s income? Last year’s? So I emailed the OMA and was given this answer:
“The base rate the parties agreed to use in our costing was FY2023/24, keeping in mind the last permanent increases were on April 1, 2023, the recent years 2.8%, 9.95% and the monthly relativity for FY2024/25 are all temporary and will end on April 1, 2026.”
Alright, some more math (my apologies). Let’s use fiscal year 22/23 to start. Let’s assume I grossed $X in that year. For FY 23/24 – that was the last year of the previous PSA and we got a 2.8% increase in fees. So I grossed $1.028X that year. FY24/25 was year I of the current PSA and we were awarded 9.95% by the Arbitrator (compounded to the 2.8%). Because there was no agreement on how to divide it up, it was distributed equally among all docs. So I grossed $1.13X.
Still with me? This year, FY 25/26, by mutual agreement, there was a relativity based increase from the original FY 22/23. FHO docs like me got 11.7% so this year, for now, I will be grossing $1.117X. This is down from last year but may change based on whatever happens in Arbitration.
Based on the OMAs reply, if FY 23/24 is the base year they used in their calculations (when I made $1.028X) then and increase of 13% on that will translate to $1.161X. In essence, if FHO+ goes through, it will mean a 4.4% increase for me next year, compared to this year (1.161-1.117) and a mere 3% more than last fiscal year. Better than nothing? Sure. Is it the major dollar influx needed to save family medicine? I think you know the answer to that.
Graph showing a hypothetical growth in gross income for a category “B” family physician who billed $350,000 in FY 22/23
2. How will rural medicine fare?
One of the things that strikes me about this model is that effectively, rural medicine will not do as well. Now, in fairness, there are attachment bonuses for taking on new patients, and those bonuses are higher in rural areas. So there is that. But my understanding is that rural doctors are working overtime anyway and not really able to take more patients right now.
But what should be noted is that in the OMA calculations, the assumption has been made that doctors are getting at least some access bonus currently. So let’s look at Dr. Rustic and Dr. Metro, a rural and urban doc.
Dr. RusticDr. Metro
Let’s assume they also fall into category “B” as per the OMAs example. It is well known that urban doctors, despite how hard they work, have challenges getting the access bonus. Dr. Metro currently gets an access bonus of $0 because there are five walk in clinics with 15 minutes of her office. This is despite her group working after hours care. Dr. Rustic on the other hand, gets $25K in access bonus, mostly because his group is the only game in town.
With FHO+ the access bonus gone and repurposed to pay for other items (and that is a very good thing as my friend Dr. Mark Linder pointed out) in effect, Dr. Metro’s raise will be $25k MORE than Dr. Rustic’s. I don’t begrudge Dr. Metro the income, she deserves it. But in order to recruit in rural areas, we’re going to have to find a way to bump Dr. Rustic’s income more.
3. What exactly will the Accountability Metric be?
This is of course, the great unknown. These metrics are often presented as “reasonable” and then governments always find a way to make them unreasonable. We won’t know the answer to that until after Arbitration.
Final Thoughts
At the end of the day, I think family doctors as a whole need to realize that FFS family medicine has gone the way of the Dodo bird (I know this will upset some FFS purists). The government also seems to recognize this and as part of the agreement is increasing the number of FHO+ positions.
Dr. FFS, Family Physician
Despite some of the concerns above, I do think that FHOs should migrate to the new model. It is slightly more money, and I do wonder if by tweaking your practice more – the amount can go up. For example, I have about 200 patients whom I have not rostered because of outside use issues – I would now roster them – and this would increase my income even more. So I suspect there is potential to make more than a 4.4% increase if you manage your roster well. Looking at increased shadow billing rates also offers some potential for more growth.
However, saving family medicine requires a multi-pronged approach that requires a single, unified health information system, family practice teams with physicians clearly placed as the leaders of the teams (with funding for leadership roles) and much more than a 4.4% increase in income. So take the money for now, but don’t in anyway shape or form believe that this in and of itself will fix family medicine.
As I write this, yet another round of Arbitration has begun between the Ministry of Health (MOH) and the Ontario Medical Association (OMA). This time, the goal is to provide a contract for years 2-4 for the Physicians Services Agreement (PSA). As was pointed out to me on social media (thanks Jane and Lisa), year 2 of this current PSA cycle began on April 1, 2025. Yet again, physicians are going to be due retroactive pay for whatever the Arbitrator decides.
Lawyers from both sides have prepared rather thick legal documents called “briefs”. (Proof number 4,638 that lawyers have a rather weird sense of humour). These briefs are public.
I’d be lying if I said that I had thoroughly understood the briefs from both sides. The excruciating agony in trying to parse the language in these things would make having a kidney stone preferable. But these are my humble thoughts from trying to do so….
The MOH team appears to have learned their lesson from last time.
To be abundantly clear right off the bat, the MOH offer for physicians is too low. They are clearly undervaluing doctors in their stance and if the Arbitrator was to accept their position, it would spell further disaster for health care in Ontario.
Additionally, the MOH has actually agreed to enhance family medicine models through the “FHO+” program, and has agreed to spend a large chunk of the funds on family physicians, an area of the health care system that is dire need. In essence, they admit that there is a problem with a shortage of comprehensive care family doctors. (NB – I will have my thoughts on the FHO+ model sometime early next week).
To re-iterate, there are still a number of problematic issues with their arbitration proposals, including the too low wage increase, the hopelessly complex method of “accountability” in the FHO+ model, a laughable statement that attachment bonuses for Complex patients will begin on July 1, 2025 when the Arbitrator won’t even rule on this until September or October of this year.
But their position is at least not stupid, and certainly not enough to make me go off like last time.
MOH Negotiations TeamMOH Negotiations TeamMOH Negotiations Team
2. The OMA Disappoints With Their Brief
Once again, to be fair, there is a lot to like in the OMA Brief. There is a good analysis of the economic picture in Ontario, a great analysis of the the delays in care, the crisis in family medicine, hard hitting information about the challenges of recruiting and retaining physicians, superb advocating to relieve the admin burden and a clear explanation of why many Alternate Payment Plans are outdated.
Alas, there is once again a “but” here…..
All of the above is what one should expect from a representative organization. One should however, also expect that organization to advocate strongly to make sure their members get their increases in a reasonable time. And it’s here that the OMA falls (badly) flat.
One of (if not THE biggest) issues for physicians these past couple of years has been the constant delays in getting the increases the Arbitrator awarded them in a timely manner. Just recently the MOH unilaterally announced a delay in paying the retroactive funds owed physicians. This is amongst a series of delays all attributed to an ancient and decrepit computer system at the government. (They’ve been making this statement for well over a decade, and very tellingly, have NEVER bothered to upgrade their system).
While the last 4 pages of the OMA Arbitration Brief does a nice job of outlining the issue for the Arbitrator, including the consequences of the MOH incompetence (physicians will simply stop doing certain procedures), the remedy the OMA seeks is milquetoast at best. From the Arbitration brief (edited):
“As a result, the OMA requests, as is normal and customary, that this Board of Arbitration remain seized with respect to any issues arising from the implementation of this Award……….“
“….with the OMA reserving its right to seek appropriate remedies (e.g. interest) in the event that the Ministry fails to meet agreed upon or directed implementation dates, particularly where the Ministry is unable to provide justification for any delay, or otherwise where the delay is unreasonable and unwarranted.”
That’s it?? All this means is that WHEN (not if – we all know the MOH can’t get their act together) the next payment delays show up, all that will happen is the OMA will complain to the Arbitrator, then there will be more hearings, and those hearings will go on for months/years and then finally, the Arbitrator MAY announce penalties to the MOH. The only good that will come out of this is that a bunch of lawyers will get rich going to repeated hearings.
What’s worse is the OMA readily admits they know the Arbitrator “favours accountability measures” in their video on the new FHO+ model (around the 3:36 mark). So doctors have to be accountable to follow an agreement, but the MOH can wiggle out and delay? The OMA can’t advocate for accountability to go both ways?
EVEN worse is that in reading the MOH briefs, they actually clearly lay out what accountability measures they want from physicians. Page 92 specifically outlines what accountability they expect from family physicians in the new FHO+ model, and how the penalties will be implemented if physicians don’t meet those accountabilities. No “seizing of the Arbitration Board” or any such thing. Now I disagree wholeheartedly with the MOH stance on this – but at least they clearly outlined what remedies they are seeking without the need for further drawn out processes. The OMA couldn’t have done the same thing??
Overall, this Arbitration hearing appears less contentious than last time, and the gap in asks is smaller overall. Hopefully this means a quicker resolution. But while there is a lot of good stuff in the OMA brief, it’s hard not feel let down by the subservient, almost nonchalant attitude the OMA is taking on payment delays. Sure looks like a golden opportunity to address this was missed.
As I write this, it appears that once again, the Ontario Ministry of Health (MOH) and the Ontario Medical Association (OMA) have been unable to agree on a contract for physicians. We are again heading for Arbitration on June 30, with hearings all next week. A slim chance exists that a last minute deal will be struck – but I highly doubt it.
The MoH and OMA Negotiating
Up until now of course, the negotiations have been held under a strict cone of silence. There is no public knowledge of what has really been said between the two sides. But Arbitration in Ontario is public. The MoH and the OMA will have to publicly disclose what they are asking the Arbitrator to award.
Some Things to Remember:
These arbitration hearings are a continuation of last years hearings. Last year the Arbitrator only set an award for the total dollar amount to be given to physicians for the FIRST YEAR of a four year contract. This year’s hearings were originally slated for March of this year, but the Arbitrator delayed them until June. He wrote:
“The issues discussed have been far-ranging and include various implementation matters, the allocation of the Year 1 targeted funding, and complex and significant physician compensation issues for Years 2, 3 and 4.”
and:
“…the Board of Arbitration is now directing that the arbitration proceedings over any remaining Year 1 targeted allocation issues, and over physician compensation and all other issues for Years 2, 3 and 4, now take place over four days during the week of June 30. ”
These hearings will be a lot more complex than last years, and will have a lot of moving parts. Not only will the Arbitrator decide on how much of an increase will be allotted to physicians in years 2-4, but he will decide on how the targeted funds are distributed. Remember that 30% of the year one Award (approx $480 Million) was to be “targeted” for areas of health system need. Because of the malignant obstinacy of the MOH’s negotiations Team, the OMA and MOH have not arrived at an agreement on how to distribute these funds. So now the Arbitrator will rule on that.
Not only that, but there is the issue of how much of an increase each specialty should get. There was general agreement between the MOH and OMA the last couple of times that 25% of any increase would be given to across the board raises for all members, and the remaining 75% would go to relativity based increases. But the two sides have never really agreed on how the 75% would be split between various specialties. Reading the statement from the Arbitrator makes it sound like he will decide that too this time. (Of course now that I write this there probably will be yet another process announced after this which will mean more negotiation and arbitration).
Last year by my very rough count, the OMA and MOH submitted over 1,400 pages of documents (ironically called “briefs”) just to determine what percentage increase should be given to physicians. I can’t imagine how big the “briefs” will be this time. I won’t be able to go through them without gouging my eyes out but I do know what we should be looking for.
Has the Ministry of Health’s Team Smartened Up?
Look, both sides are going to “posture” for the Arbitrator. As part of that, the MOH will significantly undervalue physicians and offer a pittance. We should expect that and NOT get all worked up about it.
MOH Negotiations Team Member Bob BassMOH Negotiatiations Team Member Craig RixMOH Negotiations Team Member Dr. Darren CargillMOH Negotiations Team Member Dr. David Price
A Court Jester who, given the accuracy they present, could probably be a great MOH Spokesperson
It will also be telling when reviewing the MOH briefs exactly where they feel health care is most lacking in Ontario. Do they propose more investments in family medicine? How much for each specialty? In the last couple of negotiations the MOH has tried to alter the Family Health Organization (FHO) contracts on how family doctors are paid. What changes do they propose this time?
Finally – it will be VERY telling how the MOH wants to spend the $480 million in targeted funds. Will they try to skirt paying physicians for it? For example, will they propose to pay certain physicians to hire an allied health care practitioner, saying “well it will reduce your workload”, all the while demanding copies of proof you are paying that person in triplicate? Or some such thing.
I appreciate the above may sound far fetched, but the MOH Team has proved itself to be so incompetent and borderline vengeful that a scenario like that wouldn’t surprise me in the least.
What About the OMA Briefs?
In comparison, the OMA’s job is relatively easy. They simply have to advocate for increases that will make each of their many sections 100% satisfied and not complain……
OMA Negotiations Chair Dr. Nikolina MizdrakOMA Negotiations Counsel Howard GoldblattOMA Negotiations Counsel Steve Barrett
In all seriousness, OMA briefs will also tell the profession a lot. I imagine each of the sections of the OMA will pour through the documents and send information to their members. But in short order we should all see how much of an increase the OMA has concluded each specialty warrants, and how the OMA plans to handle the perpetually thorny issue of relativity.
Additionally, the OMA has repeatedly point out that we have a shortage of comprehensive care family doctors. They’ve used the word crisis more than once to describe this. So as a family doctor, I am eager to see what changes they propose to the FHO model as well.
Most importantly, will the OMA be aggressive in defending its members? These last couple of months had seen absolutely unacceptable unilateral decisions by OHIP, delaying payments to physicians and making mistakes on their remittance . The OHIP bureaucrats blame their old outdated computers. Of course, when they plan to recoup the 9.95% they overpaid for the preventive care bonuses this past month – the OHIP computers magically managed to figure out how to get the money back immediately.
Will the OMA finally demand in their Arbitration briefs some sort of penalty for OHIP screwing up? Remember, the fee changes as a result of this contract are to come into effect on April 1, 2026. Given the Arbitrator likely won’t hand down a ruling until the fall, there is no way OHIP will get their act together in time without……..encouragement. Penalties/Interest for delayed payments should absolutely be demanded by the OMA.
All in all, next week, physicians will learn just how both the OMA and MOH feel about them. Buckle up folks……
Last week, a study published in the Annals of Family Medicine revealed what those of us in medicine knew all along. More and more, physicians who are trained in comprehensive family medicine, are choosing to do other things. There are a myriad of reasons for this (ranging from poor remuneration, lack of respect from government, incredible admin burden and more). But the blunt reality, which is very very bad for the people of Ontario, is that despite having enough family doctors, not enough of them are practicing comprehensive care family medicine, and more are expected to stop.
There was of course, a large amount of press interest in the study, and rightfully so. Probably the best interview given by one of the studies authors was by my friend Dr. Kamila Premji (who is brilliant) and can be listened to here.
I was fortunate enough to be asked about this issue last week on “Toronto Today” with host Greg Brady. As I explained to him, I personally am left with decidedly mixed feelings about the report.
The Hope
It’s not like people haven’t been talking about this for a long time. Heck I wrote about how Ontario does NOT have a shortage of family doctors, just over a year ago. I pointed out that family doctors were leaving to do other things then.
But now that there is a comprehensive study done on the matter, maybe, just maybe, the bureaucrats at Ontario Health will finally do something positive about the matter. (I won’t bet the mortgage on it – but there is a teensy little bit of hope).
All of these doctors were ignored. When Dr. Alam wrote her blog, “only” 800,000 people in Ontario didn’t have a family doctor – we are over 2.5 million now.
Thinking about how much better off we would be if the bureaucrats at Ontario Health hadn’t unilaterally ignored these doctors makes my blood boil.
The Fear
Which brings me to my biggest fear in all this. When I look around at some of the Ontario Health staff, and see some of the reports/decisions and directions given by various committees/panels/departments of Ontario Health, I see frankly, a lot of the same old names and faces. The same bureaucrats that ignored Dr. Alam and others for over a decade, and have made bad decisions and recommendations ever since, are still in charge. Many have been promoted. All of them are going to retire with full pensions. And yet now, they will likely be tasked to find a solution to the very mess that they failed to foresee and in many cases aided and abetted in creating.
If I may paraphrase Albert Einstein a little bit, to expect the same people who consistently and repeatedly made wrong decisions over the past ten years to suddenly not make a mistake with the next set of decisions is surely the definition of insanity.
So What’s Next for Family Medicine in Ontario?
As I think most of us know, Dr. Jane Philpott has been tasked by Ontario Premier Doug Ford to lead the new Primary Care Task Force. Her stated goal is to ensure every resident of Ontario has primary care within the next five years. She has a strong relationship with Dr. Tara Kiran, one of the more visible authors of the study on family doctors. Both seem to be working closely together.
Dr. Tara KiranDr. Jane Philpott
Both of them seem genuinely passionate in their support of family medicine. They also understand the foundational importance of family medicine in a strong health care system. I believe they both have the desire to fix this crisis as soon as possible. We should all want them to succeed, because success means a healthier population for all Ontarians.
But…..
To date, I haven’t seen in either of them the willingness/ability/chutzpah/brass necessary to tell off our woefully incompetent bureaucrats at the Ontario Health and tell them which direction we need to go in. As I mentioned above, we just cannot rely on the advice the bureaucrats are giving anymore – nor the processes they have put into place.
One small example of ongoing bureaucratic incompetence if I may. It’s been know for over fifteen years now that our health care IT systems are completely disorganized and don’t talk to each other. The situation is so bad that healthcare is the ONLY major industry in which fax machines are still used (seriously). It’s so wasteful that it’s been estimated that we could save $2.1 billion dollars a year if we unified our health IT systems. (Which ironically is about how much Dr. Philpott has been given to fix the family medicine crisis).
Recently, Ontario Health announced that it would develop an electronic referral system to get rid of faxes. Sounds great. But unfortunately, a deep dive of their plan suggests that each of Ontarios 180+ health teams is to pick their own software. Which means you could have a situation for someone like myself, who has patients from two different areas, being forced to use two different electronic referrals systems. Which will do absolutely nothing to reduce my admin burden, the same admin burden that the study’s authors admit is driving physicians away from comprehensive family practice.
The family medicine crisis desperately needs to be fixed in Ontario. It will take a combination of a seamless electronic record system, processes in place to reduce paperwork, increased pay for family doctors (including pay for admin work and retention bonuses) and yes teams where the family doctors guiding them. But I don’t think any of that can happen until we clean out the bureaucrats at Ontario Health.
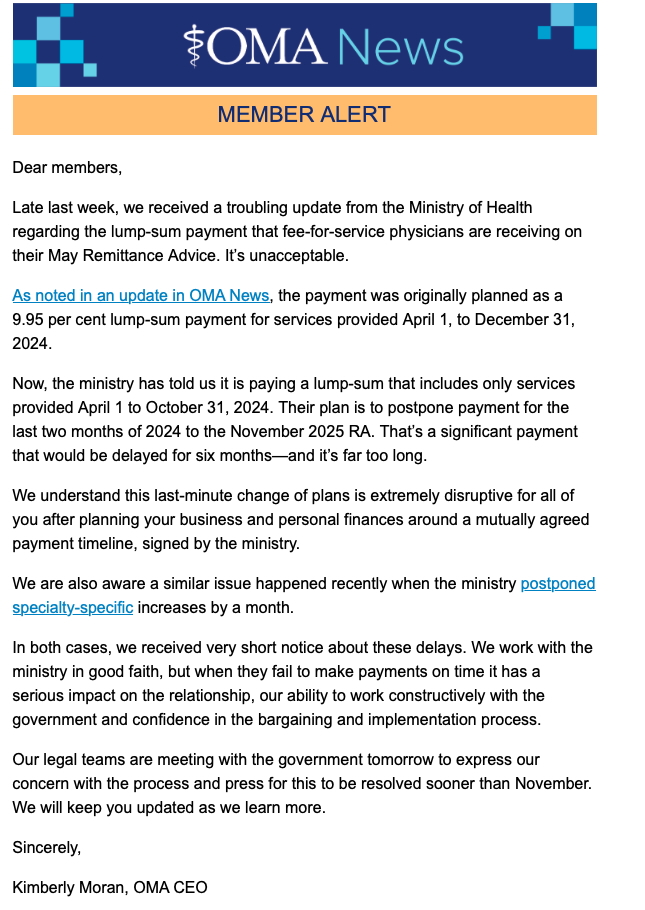
Last Friday (May 2), in what was a classic Friday afternoon bureaucratic dump, the OHIP bureaucrats at the Ministry of Health announced that they wouldn’t be paying the full amount of back pay owed Ontario’s doctors, as per the arbitration award. This was a unilateral decision on their part. It was contrary to what was in a signed agreement, and the OMA Board was notified at the last minute. (OMA CEO Kim Moran’s email is attached to the bottom of this blog). The bureaucrats promptly ran away an hid for the weekend hoping this issue would go away (kind of like how Sam Bennett cowardly hid from the press after putting an elbow to Leafs goalie Anthony Stolarz head).
This is, in my opinion, the latest attack on physicians as a whole from Ministry of Health (MOH) bureaucrats, who clearly are more interested in trench warfare than working co-operatively with Ontario’s doctors to improve health care for the citizens of Ontario. Don’t believe me? Consider the following:
The bureaucrats had the option of realizing that provinces like Manitoba/BC/Saskatchewan and even Alberta(!) recognized the need to work with their doctors and come up with a funding formula for them. Instead they chose to drag Ontario’s physicians through a protracted (going on three years now) and highly antagonistic arbitration/negotiations process.
Not only that, in response to now multiple stories of people lining up to find a family doctor in the press, their response was that there was “no concern” about the shortage of comprehensive family care physicians. (Seriously, how out of touch must they be to think that that type of Orwellian double speak is going to work in Canada).
People lined up hoping to get a family doctor in Walkerton. Photo originally posted in the farmers forum.
Frankly, this inept, combative and dismissive treatment of physicians is just par for the course for this bunch of bureaucrats. It saddens me, but it doesn’t surprise me.
No blame for this decision should fall to the OMA. They did negotiate a signed agreement (as per Ms. Moran’s email) and they clearly were not notified about the unilateral change until far too late. So the unilateral action is not their fault.
But….
What the OMA can, and should be held accountable for is how they proceed from here.
I don’t want to seem overly difficult here. If I truly was an obstinate person, I’d try to get a job at the Ministry of Health – perhaps on their Negotiations Team. The reality is that I actually have a long history of working co-operatively with government to improve health care in my neck of the woods.
I’m serious. In 2001 I helped bring in the first stage of Primary Care Reform called the Family Health Group. In 2004 I was one of the lead physicians who brought in a capitation model of payment for family physicians (it was initially a Family Health Network and it eventually evolved into a Family Health Organization). From 2007 -2013 I was the founding Chair of the Georgian Bay Family Health Team and From 2013-2015 I was the Health Links lead physician in my area.
And in each of these roles I worked closely and co-operatively with government to try to improve the health care needs of the patients in my area.
But – in those days, the bureaucrats wanted to work with doctors. They wanted to co-operate to improve health care and they were genuinely concerned about the lack of family physicians providing comprehensive care. They didn’t want to play power games with physicians or harass them or do dumb things like the current crop just did.
It’s important for the OMA to (finally) realize that there really is no hope that they can work with the current lot. They’ve already dragged us through three miserable years of negotiation/arbitration and fought us (thankfully often times stupidly – as even the Arbitrator pointed out) – for the sake of…….. I don’t know why really. Maybe it’s a power play? Maybe there are just bullies?
Recognizing the obstinance of the MOH bureaucrats is why I was proud (and still am) to have my name on an Op-Ed in the Toronto Star last year advising Family Medicine Residents to NOT start a practice in Ontario at this time. But I have to tell you the blowback from the OMA was saddening to me. I will not mention names – but one senior exec told me that the OMA was working well with the Government. Worse, one senior physician leader texted me the following:
Text from a very senior physician leader at the OMA
Remember – at the time this text was sent to me – we had already been locking horns at the negotiations table for two years and the government had done absolutely nothing to solve the family medicine crisis. Perhaps the physician leader felt the relationship was “best ever” because at least they weren’t sabotaging doctors left right and centre like the abhorrent Eric Hoskins did.
Despite all of that, there was some movement forward with arbitration. While no where near what other provinces got, it at least recognized the need to fund health care better, and provided hope for funding for offices, clinics, and frankly other badly needed resources.
Now the MOH has decided unilaterally to not pay, or pay whenever they feel like it, so we are back to – do NOT start to work in Ontario.
At any rate – as mentioned, while the OMA cannot be judged on decisions by the Ministry, what the organization does next will be telling. Will they finally recognize that the current lot of bureaucrats simply cannot be dealt with by reason? Will they recognize that physicians are essentially being bullied by these ruffians and the best way to deal with a bully is to stand up to them? Will they take legal action (according to Ms. Moran’s email – there was a signed agreement which the MoH is now in violation of)?
I don’t know the answer to any of the above. But I can only hope that the current Board recognizes that there is no hope of working in good faith with this lot of bureaucrats and that strong, frankly militant actions, are needed to support the members.
Addendum: After I published my original blog, an anonymous colleague asked that I publish a link to a survey about this issue. I’ve therefore appended my blog and ask all Ontario physicians to click on the link below and honestly reply to the questions:
Congratulations on winning the last election and being re-appointed health minister. The health ministry is the toughest job in government. I sincerely mean now, what I wrote before, that all of us should hope you are successful. Ontario deserves the healthiest possible population.
Of course, that still won’t stop me from giving you advice (whether you want it or not)……
I’ve noticed that you place a really high value on making sure that health care is “convenient.” Your government even calls the overall program “A Plan for Connected and Convenient Care.” Your talking points in the press always mention “convenient.” Even the second major outline for health care uses that word.
I would suggest that rather a lot of your health care platform is based on making people happy by giving them what they want and making things easier for them. For example, your boss, premier Doug Ford, when talking about the expanded scope of practice that allowed pharmacists to prescribe treatments for minor ailments focused almost exclusively on the fact that it was one of the most popular things your government has ever done. The public was satisfied, so it must be a good thing.
Now I appreciate that you don’t have a health care background. If you did, you would know, that convenient health care, and patient satisfaction in health care, actually have a negative correlation with health care outcomes. Essentially, when patient satisfaction with the health care system goes up, the health care outcomes get worse. A study published in Medscape showed that focusing on patient satisfaction lead to 12% higher hospital readmission rates, 9% higher health care costs and 26% higher mortality rates.
Basically, focusing on convenience and satisfaction in health care costs more, makes people sicker and kills more people.
However, at this point, I doubt that I can get you to shift away from this philosophy. So I have an idea that will make health care much more convenient for people. Something that will reduce the amount of travelling back and forth that people do, and will allow them to quickly and easily get their health care needs taken care of in one spot.
How will this be convenient? Well, right now, when a patient goes to see a physician for, let’s say high blood pressure, the patient will get assessed by their family doctor, and based on their medical history, an appropriate medication will be chosen for them. They will then drive to the pharmacy with that prescription. The pharmacy will take however long it takes for them to fill out their prescription, and after a period of waiting, the patient will get their needed medication.
By allowing physicians to have their own dispensary, a patient will now go to the physician’s office, and if a prescription medication is deemed necessary, they can just purchase it from the physicians office right then and there. It saves them an extra drive, and perhaps even parking lot fees depending on where they go. This will, of course, be extremely convenient for the patient.
What’s that you say? Isn’t this a conflict of interest? I mean, if a physician is now able to sell the drugs after making a diagnosis, wouldn’t it encourage physicians to prescribe more medications?
Um, can I ask why that didn’t seem to bother you when the pharmacists were allowed to expand the scope of their practices by you? Pharmacists now make an assessment for certain minor illnesses, get paid to do that by the government, determine what in their opinion the right treatment is, and then sell the patient the drugs at a profit. (This is what naturopaths and some chiropractors do as well, but that’s a whole other story.)
What’s that you say again? Pharmacists have to abide by a certain code of conduct from their college. They are bound by their code of ethics to act in the best interests of their patients. Um, ok. You do know that physicians also have a college that we answer to, right? You do also know that physicians also have a code of ethics? That we all took an oath to do no harm to our patients?
Might I ask exactly what the difference is between these two scenarios?
Of course, while most patients would be happy for this convenience, I imagine not everyone will be happy. I suspect (Shoppers Drug Mart bigshot) Galen Weston would be quite annoyed if you did this. But hey, look at the bright side, at least you won’t have to deal with some miserable crotchety old country doctor spouting off in the media wondering who exactly the health minister was in this province.
Galen Weston, of Shoppers Drug Mart and Loblaw fame.
Look, at the end of the day, for me, it’s health care outcomes that matter the most. I want patients to have the best possible results for themselves and health care as a whole in Ontario. But if you are going to insist on “convenience” then at least do it in a way that’s fair to all of the health care professions.
Change or amend the 1991 Medicine Act to make life a little easier for the patients.
Yours truly
An Old Country Doctor
P.S. While you’re at it, don’t forget to direct your OHIP Bureaucrats to not seek repayment from Dr. Elaine Ma. Don’t think doctors in Ontario have forgotten about this situation.
Canadians are currently dealing with the dizzying spectacle of Donald Trump’s tariffs against our country. On again? Off again? Delayed? Doubling? I’ve personally gotten seasick trying to keep up with whatever tangerine Palpatine is thinking.
U.S. President Donald Trump – aka the Tangerine Palpatine
However Canada’s response to this (and the nonsense about us becoming the 51st state) has frankly been quite lacking. Yes, it’s great to see Canadians being able to fly the flag with pride, especially after the miserable co-opting of the Canadian flag by the freedom convoy types, who likely themselves were Donald Trump supporters. (How’s that working out for you guys now?) Yes #elbowsupCanada is a wonderful approach to take and a great mantra going forward, particularly with how intertwined hockey is with our nation. (Quick reminder: Not only do we win Olympics, we win Four Nations Cups as well).
Four Nations ChampsMens Olympic GoldWomen’s Olympic Gold
BUT, for all the outcropping of (absolutely warranted) national pride – our governments – outside of launching retaliatory tariffs, haven’t done anything to fix the systemic problems in our economy. For example, getting rid of domestic trade barriers and having free trade between provinces would provide a boost of up to $200 billion dollars to our economy, but seemingly no action on this yet.
Even more importantly and what’s long overdue, is an absolutely necessary look at the bureaucracy and impediments that many businesses face in trying to contribute to our economy. Let me talk about a personal experience (and no disrespect intended to the good people on staff in my township).
About 10 years ago, our community had clearly outgrown the medical centre. Some poor sap was put in charge of expanding it. (Guess who.) I had to deal a myriad of problems of putting an addition on our medical centre. Here’s a couple of examples of what I dealt with.
As per policy, the township requested that we provide an engineered site plan. The reason for this was to assess water drainage requirements. While on the surface this makes sense, all the engineered site plan was going to tell us what size of culvert to put on our property for water drainage. The estimate for the site plan was about $15,000.
A sad, lonely culvert, passing its life away draining water…
However, it turns out there were only two sizes of commercial culverts for our project. A big one and a small one. The big one cost $500 more than the small one. Being well-versed in the obstinacy of Ontario Health’s bureaucrats, but somewhat naive in the inflexibility of municipal bureaucrats, I offered to simply put in the bigger culvert right from the start in exchange for waving the engineered site plan.
Those discussions went as well as my less naive readers will expect. The site plan wound up costing $17,000, and it told us that we had to put in the big culvert.
Want more? The township requested a $250,000 letter of credit or certified cheque prior to approving the expansion of the building. My initial reaction was somewhat negative to this request, but upon reflecting, I did realize that it made sense. The request was put in place in case a builder started a project, ran out of money before they finished the project, and left a hole in the ground. The money would then be used to pay to clean up the mess they made.
I still grumbled about the fact that the township was making long term doctors who were clearly invested in the community do this, but I have to concede that it was fair.
The bank informed me there’s some complex fee formula for a letter of credit – and it would have cost $5,000. I asked them for a certified cheque, and it turns out banks don’t do that anymore. However, they were willing to issue a bank draft and the fee for that was $50. Obviously, I got the bank draft instead.
When I went to the planning office however, I was told this was unsuitable. The contract we signed specifically asked for a Letter of Credit or Certified Cheque and I had presented neither. Therefore we had not met the terms of our contract and the project would come to a halt. The staff person did offer to take this to the planning committee, and six weeks later they decided this was ok.
Is this me just griping? Nope – in fact his is happening all through health care and businesses in Canada. I recently spoke to the owner of a Nursing Home. His home had been approved on a “fast track” for a new build based on the dire shortage of nursing home beds in Ontario. I asked when the facility would be built and he just laughed. Apparently “fast track” means that there will “only” be 30 months of paper work (!) before the shovels go in the ground and he hopes it will be completed in 5-6 years!! I’m guessing this “fast track” must be on Toronto’s Eglinton LRT line….
A sad, lonely train on Toronto’s much, much, much delayed Eglinton LRT line
Want more? Just look at the saga of my local hospital, the Collingwood General and Marine. We’ve known for almost two decades that it’s far too small for the community. Heck the community has been asking for a new hospital since the early 2010s and finally got approval on phase 1 (of 5) in 2016. And 9 years later (!) we are at phase 3. The “hope” is that the new building will open its doors in 2032 – 16 YEARS after it was absolutely clear a new hospital was needed immediately.
New Prime Minister Mark Carney is off to Europe this week to build trade and strengthen relations. Nothing wrong with that, we need reliable trade partners in the future. BUT, we face an unhinged, hyper volatile situation with our neighbours to the south RIGHT NOW. It seems to me there is no better time than now to drop intra Provincial trade Barriers and right size the bureaucracy allowing for businesses to grow and thrive more easily in Canada. As for health care, the right time was 10 years ago.
Last week, I had the opportunity to talk to Greg Brady, on his 640 am radio show, Toronto Today. The episode is on Spotify and, if you are in need of a great cure for insomnia, you can catch me starting from about the 19:30 mark:
Six and half minutes is not enough time to discuss health care in Ontario. Neither is a 1,000 word blog, but that won’t stop me from trying to expand on some of my thoughts.
The first and most prevalent thought I have is disappointment in ALL of the political parties for how they have addressed health care so far. Everyone on the front lines of health care has known for a least a decade that we need bold transformative changes in how health care is run and delivered in Ontario. Probably all of Canada.
And yet, the four would be Premiers all fail to outline a plan for such transformation. Instead, they have all resorted to that age old political vote grabbing stunt of saying “Let’s just throw more money at the problem” without actually reminding you that the money is going to come from YOUR pockets and is going to be, frankly, poorly spent.
Liberal Leader Bonnie CrombieGreen Party Leader Mike SchreinerConservative Leader Doug FordNDP Leader Marit Stiles
The Conservatives hired Dr. Jane Philpott to oversee a spend of $1.8 billion in a plan to connect everyone with a “primary care provider” in the next few years. As I’ve written before, that plan, through no fault of Dr. Philpott, who I have a great deal of respect for, is doomed to failure.
The Conservatives did not start the downfall of family practice in Ontario (that was the miserable Eric Hoskins/Bob Bell duo during the wretched Kathleen Wynne years). But they sure haven’t done enough to fix the mess they inherited. Economist Boris Kralj, PhD, recently showed in the Medical Post that Ontario lost 238 family physicians in 2022/23 – the biggest loss of any province.
Former Premier Kathleen WynneFormer Health Minister Eric HoskinsFormer Deputy Health Minister Bob Bell
The Liberals for their part want to spend 3.1 Billion dollars. At least they promise everyone a family doctor and not a “provider” (and yes, there IS a difference, a BIG one between the two). However, their plan amounts to spending $1.3 billion more than the Conservatives. Spending more without changing things seems naive at best.
The NDP promise to recruit 3,500 more doctors, promise family doctors for everyone, cut red tape, establish a “Northern Command Centre” for health care (that’s actually a good idea) – all for the low low price of only $4.1 Billion dollars, a billion more than the Liberals.
The Green Party promises are actually the most detailed I could see, including lots of goodies, like recruiting more doctors, building more nursing homes, increasing nursing student spots, hiring 6,800 personal support workers and more. There is only one thing missing from the proposal (at least on their website). How much this will all cost YOU, the taxpayer.
Ontario spends $81 billion in taxpayers dollars on health care. Rather than look to see if that money is being spent wisely, and looking to transform health care, all the political parties are simply giving us sound bites. They promise to spend $83-$85 billion on the same failing system, without looking at changing things. Because spending more inefficiently will surely fix things.
OK Smart Guy – What do YOU Think Should Be Done?
Glad you asked dear reader, glad you asked. At an absolute minimum I’m looking for a party that has the political courage and wisdom to do the following three things.
First,A complete hiring freeze on all bureaucrats in health care, including not replacing those who retire, or leave for other reasons.
Currently Ontario has 10 times as many health care bureaucrats per capita as Germany. That’s too many. This means that any meaningful suggestions for change have to go through so many bureaucrats that the whole system is plagued with paralysis by analysis. Time to trim the fat.
Second, ensuring one, and only one, patient app that every resident of Ontario has, which will have access to all their health care data, and allow them to share this with the health care specialist or facility of their choice
Ontario is a digital health nightmare. Your health information often times can’t be shared if you go from one hospital to another, or one doctor to another. There are multiple inefficiencies and unnecessary repeat tests because of this mess and it should never have been allowed to occur.
It would be too expensive and too time consuming to force every health care facility to use the same electronic medical records system. What can be done however, is to force all the systems to integrate with ONE patient app. This will ensure a common standard, and moreover will allow a hospital you happen to be in, to access your out patient information (with your permission) which just doesn’t happen now.
Third, ensuring strong family physician representation at the board level of the Ontario Health Teams.
There is a lot of talk about the benefits of team based care. As someone who views one of his proudest achievements to be the founding Chair of the Georgian Bay Family Health Team, I would agree with this. The current plan for Ontario Health Teams does have merit. BUT, in order for these teams to succeed, they need strong family physician leadership at the GOVERNANCE level. That’s right, you need to put doctors (and more than just a token one) on the Boards of these teams and ensure the teams are led by them – for best clinical outcomes. I don’t see that in the plans.
Final Thoughts
My usual followers will know that I generally vote on the conservative side of the political spectrum (de gustibus non est disputandum). However, I’ve been frankly disappointed that the current Conservative government has been anything but conservative. Sadly, the other parties are really not offering the kind of transformative solutions we need in health care either. I firmly believe that we should all vote in elections, and I certainly will, but for now, call me an undecided old country doctor.