Recently, there’s been a lot of talk about the “administration burden” faced by family physicians. The Ontario College of Family Physicians estimates family doctors spend up to 19 hours a week on “paper work”. Given there are only so many hours in a week, the more hours spent doing paperwork, the less hours seeing patients.
It also contributes to situations where people just get too frustrated with family medicine, and quit. Twenty percent of Toronto family doctors are planning on leaving within five years. This bad karma is not lost on medical students, who, as I mentioned in a previous blog – are avoiding family practice like the plague, worsening a crisis that has been years in the making.
But what exactly is this “administration burden”? What’s the “paper work” that is driving us all to frustration? I would argue it’s not paper per se, it’s digital.

That’s not to say there isn’t paper. I frequently get asked for completely pointless sick notes from employers, impractical forms to return to work and seemingly useless – “we agreed your patient was permanently disabled, but we want a one year update to make sure your patient is still permanently disabled” forms from the pointy headed bureaucrats at insurance companies. But I’ve taken a somewhat mercenary approach to those forms in order to keep myself sane.
A sick note costs $20 and takes about a minute to write. A form the insurance company asks for usually takes a few minutes to fill out and I charge $40-$175 depending on the form. I reconcile the fact that these forms are a burden, with the fact that at least I make money out of them. While somewhat unscrupulous on my part, it keeps me from totally blowing my lid whenever I see one of these.
No the real admin burden comes from the completely absurd and unrelenting avalanche of reports/lab work/follow up notes – all of which present to me in a haphazard way, seemingly designed to drive me to psychiatric medications.
I took the Friday of Eid ul Fitr off to celebrate with my family. On Saturday, I logged into my Electronic Medical Record (EMR), correctly realizing that if I waited until Monday, the EMR inbox would crush my sorry soul.
Unsurprisingly, I had a total of 75 labs/reports/messages about patients to review. It wasn’t so much the number of items to take care of, (truly if they were straight forward it wouldn’t have been too bad). It was rather how badly and inefficiently the information came to me that sucked all of the happiness I had enjoyed on Eid from my spirit.
One method of getting information to me is via a system called Hospital Report Manager (HRM). I look at HRM in my EMR and see a report on a renal transplant patient from Sick Kids. But the note was “uncategorized” which meant that I had to go into the HRM software and enter the category “nephrologist” in the report. The VERY NEXT report in my HRM in box was……the exact same report on the exact same patient, but this time HRM had categorized the report as being from a cardiologist – so I had to go in, change the report once again to “nephrologist” and I now have two copies of the same report.
By the way – Sick Kid’s hospital provides exceptional medical and nursing care to my patients, but ever since they switched their hospital IT systems to a company called EPIC there has been no end of issues like this. The only thing that software is epic at is causing physician distress.
That’s not all. HRM has more goodies awaiting for me. There’s a report from my colleague Dr. Collings on his expert management of a wrist fracture on one of my patients. Thorough, comprehensive, and well done. Except HRM has auto-categorized him to be a gynaecologist So yes, I either have inaccurate information in my patients chart, or I go back and re-categorize the report to reflect that Dr. Collings is an orthopaedic surgeon.
Next up, HRM has a report from an Emergency Room physician about a patient who was seen and apparently had some abnormal bloodwork. Not life threatening, so asked to follow up with me. Only problem is the blood work from the hospital doesn’t come to me via HRM. Now I have to go to that patients chart, and access yet another system called OLIS, log into that and download the lab work from the hospital. But wait the note from the ER was unfortunately late getting to me (about 10 days out). OLIS is set up to auto download for the past seven days, unless I click more buttons, and back date – which I have to do.
Next up, a report from HRM that a patient of mine had a Covid swab done. But HRM won’t tell me if the swab was positive or negative. Just that it was done. Now I go back to that patient chart and access OLIS where the result is, adding yet more steps to my day.
Next come messages (yes, that’s on top of HRM and OLIS). I note a message from the local Shoppers Drug Mart asking for a renewal of blood pressure medications for a patient of mine. Only problem is that a brief look at the chart shows I sent a one year supply of that same medicine to the Shoppers three months ago, and they accepted this and downloaded it. I tell the pharmacy staff who tell me they “can’t find it” which leads to……well, let’s just say a deterioration in the conversation.
As an aside, while I’m not allowed to endorse any specific pharmacy, I will say I’ve generally found care to be much better when provided by smaller, independent pharmacists who build relationships with their patients, rather than big chains that just seem to fly in itinerant staff.
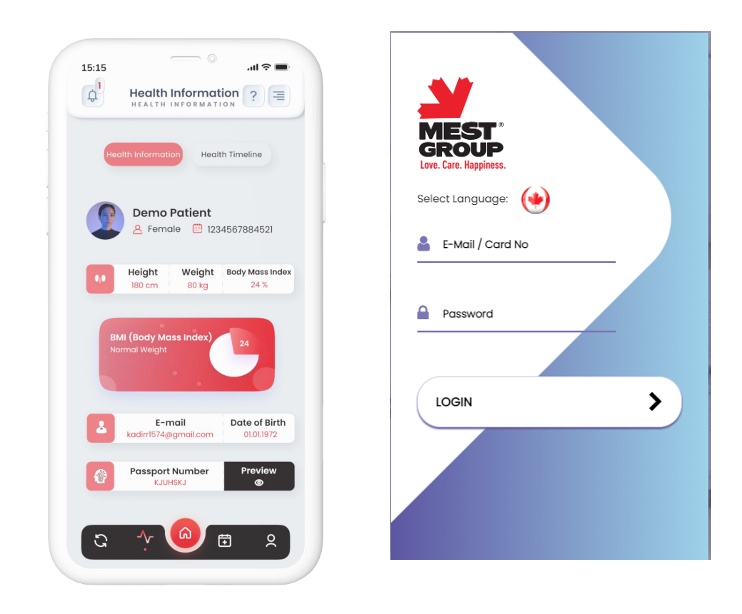
Anyway, you get the point. In total it took about 3 hours on Saturday to sort through this mess and it just doesn’t have to be this way. The reason I wrote a blog about Health IT in Turkiye was to show that other countries do a much better job of managing this burden. I’m sure there are other examples and we need to learn from them.
The vast majority of my family practice colleagues practice family medicine because they genuinely like their patients, like providing comprehensive care, value the relationships built over time and feel like they make a difference in peoples lives. But unless we do something about this administration burden, I fear more and more will leave the profession, because at some point, being human, they just won’t be able to take it any more.