

My thanks to @radioKristy from @CFRAOttawa for interviewing me yesterday about the op/ed @DocSchmadia @silvym98 and I wrote about the #crisis in #FamilyMedicine in #Ontario that ONLY @ONThealth can fix. Link below.
Open Letter to All Family Practice Residents



The following letter was jointly written by the three of us and published in the Toronto Star on February 20, 2024. It is being reproduced below so that we can share the letter on Facebook as we believe it will be of interest to physicians across Canada.
To All Family Medicine Residents,
We are writing to say congratulations! You are nearly at the end of a decade of hard work, perseverance and sacrifice; ready to start your career and “real life”. You have joined a beautiful and unique specialty. You will be the key to the healthcare system. You will find answers when patients arrive with ambiguous symptoms. Others will tag in and out of a patient’s health journey. You will stay and be an essential part of the beginning, middle and end of every patient’s story. You will save lives.
Your skill and knowledge are unparalleled, and there is no substitute for your expertise.
Which is why with heavy hearts, we, the undersigned, recommend that you do not start your own family medicine practice in Ontario. Not right now.
Family medicine is in crisis. Family doctors in Ontario are unable to provide the care they could and should. We face unprecedented levels of administrative burden, unsustainable business expenses, lack of healthcare resources, lack of social and cultural support for our patients and ourselves and finally, a lack of respect. This has led to widespread burnout and exhaustion.
In short, it is becoming frankly unsafe to run a family practice in Ontario, especially for those just starting.
We are family doctors with decades of experience. We are also physician leaders, past-presidents and board directors of the Ontario Medical Association (OMA), academic faculty, and health policy experts. We understand the situation well.
Do not sign that contract. Do not sign a lease, hire staff, buy equipment, contract with an EMR or any of the million things that must be done so that you can start a comprehensive care family practice.
Starting a practice at this time will require you to continue to sacrifice everything else in your life. If you have debt, you may not be able to pay it down, let alone start living the life you and many others have postponed for so long. You will struggle to spend time with your family, buy a home, care for vulnerable loved ones and more. You will continue to work at a non-stop pace, this time with no end in sight.
You will burn out and like many others, leave family medicine for good. This is why millions of Ontarians no longer have a family doctor.
The Ontario Ministry of Health can solve this crisis.
Governments in Manitoba, Saskatchewan and British Columbia have done so. This past year, they made family medicine a priority – and backed their words with targeted funding toward key programs to support both new and established doctors. It comes as no surprise that they have welcomed hundreds of new family doctors into their communities.
If they can do it, so can Ontario.
What can you do in the meantime? Work in hospitals, hospices, operating rooms and long-term care. Work in obstetrics, anesthesia, as a hospitalist, in emergency or palliative care, oncology, sports medicine etc. Be a locum. Bide your time.
You are skilled, smart, and adaptable. Your knowledge is extensive, demonstrating an unmatched depth and breadth of training. Use it.
When people leave comprehensive care family medicine, they almost never come back.
We don’t want that to happen to you. When the government of Ontario recognizes family doctors as the foundation of medical care, negotiates a fair contract and improves health policies to reflect patient needs in 2024… well, when that happens, we will write a different letter and welcome you to the world you were meant to be in.
We hope by then it is not too late.
Sincerely,
Dr. Nadia Alam, comprehensive care family physician and anesthetist, past-president of the OMA
Dr. Sohail Gandhi, comprehensive care family physician and hospitalist, past-president of the OMA
Dr. Silvy Mathew, comprehensive care family physician and long-term care, past-board director of the OMA
Dr. Corli Barnes on the Challenges Facing New Family Physicians

Dr. Corli Barnes , pictured here, guest blogs for me today. She is a Family Practice resident who is just completing her residency. She sent the following letter to the Sudbury media after reading reports about the crisis in family medicine. I thank her for allowing me to reproduce the letter here.
Hi Len,
I read your article about family physicians. I am a second-year family medicine resident here in Sudbury, ON, originally from Manitoba. Thank you for taking the time to help raise awareness about the crisis in Family Medicine. I wanted to write to you to offer a viewpoint not often accounted for in this conversation.
I’m about to graduate as a family physician. After ten years of climbing that Mount Everest, eight of those years without an income, paying for two full-time degrees plus inflation and living costs, I’m $350,000 in debt. That’s living on around $31,000 a year.
The government just denied me loan repayment assistance because I get paid ~$68,500 a year as a resident. The cost to write my final exam just went from around $1,500 to $4,201. When starting a practice, a monthly bill of anywhere from $7,000 to $12,000 in overhead is waiting for most grads who take up a clinic practice, plus ~$2,000 a month in interest on debt if you supported yourself through school.
When I start practice, I can expect the Ministry of Health to take it’s time (at least two months) to approve my funding model. My first paycheck will come in at fee-for-service levels that won’t cover my costs.
About a year and a half ago, after working a 60-hour week, I started to quietly panic when I did the math to project my net income as an attending physician. Clinic-based family medicine is my passion, and I realized that it wasn’t going to work out based on the way most physicians work. I wouldn’t be able to even begin to pay off my debt.
After all that work, sacrificing my twenties, my health, friendships, and enduring the stress of medical training – I wouldn’t be able to cover my living costs as an attending family physician.
Try imagining uprooting your entire life to go on a pilgrimage to a promise land and when you finally get there, it’s a shell of what it once was. A ghost town with worn out buildings and hardly anyone in sight. You’re 10,000 miles from home and way worse off than when you started.
The only promise this journey has fulfilled is providing the education necessary to safely and meaningfully help people who are sick and enable them to seek wellness.
A family doctor is the only professional that is trained adequately to be able to pick out disease from the general population. It is the only medical specialty educated in every body system, who is there to catch those who fall through the cracks, prevent disease, and deliver medicine in a way that suits an individual.
This work will always be challenging and meaningful, requiring dedication to keep up with rapidly increasing medical knowledge and motivation to continue to seek excellence. The challenge is great, and the reward for doing it well – a healthy patient – even greater. This is why I’m passionate about it, and sad to see it fall apart and go unappreciated. It’s hard to watch as its integrity is cheapened by being grouped into an emerging category of primary care providers with far less training and liability, and have its voice drown out by promises of funding that seem to keep ending up in someone else’s pocket.
Because of the way things are, I have had to pivot considerably by coming up with creative ways to practice medicine and supplement in my income in the future.
Many of my peers have elected to do emergency medicine, hospitalist, subspecialize in family medicine or locum while they contemplate their options.
With every news release, I read about funding for health teams, funding for free schooling for nurses, funding for nurse practitioners, funding for “programs to reduce administrative burden” that I have yet to see a benefit of. I open the news everyday, hoping to read something about increased pay for family physicians. Instead, I read about how negotiations are not going well with the government. I read that the planned increase of 2 or 3% has been cut down to 1% or 0%.
Sometimes, it’s hard to not regret going into any number of specialties I could have. I go to work, and I do my best to help the patient in front of me. They ask about where I’m going to practice with hope in their eyes. They leave feeling better, and I try not to think about the fact that for many family physicians, the thanks for that visit is just $12 to take home.
Eventually, fueled by the same determination that got me into medical school, I started to dig deep to find a solution that wouldn’t mean I would have to abandon my dream of opening a clinic-based practice. A solution that wouldn’t mean I have to give up freedom I’ve waited years for, work unsustainable hours or in a toxic environment bred by chronic underfunding.
I scoured Ontario looking for a place that would help fund the start of my career in a meaningful way while having a sustainable business model that supports good medicine. After around a year of this search, I am lucky to have found a place in Madoc, Ontario but I can report that it is a very hard thing to find.
I am sad to be leaving Sudbury, where I currently live and initially hoped to call home when I moved here in 2022. I hope this letter helps to raise awareness about the difficult situation many residents are in and how urgently family physicians need change.
Actually, Ontario Does NOT Have a Shortage of Family Physicians….

You’re probably wondering if I’ve lost my mind. The media is currently littered with stories about how 2.3 million people in Ontario don’t have a family doctor and how that number is expected to double in two years. Family practices are closing down. In Sault Ste Marie – over 10,000 people are about to be orphaned (left without a family doctor). The Ontario Union of Family Physicians just held an event geared towards helping family doctors leave the profession.
How out of touch must I be to make the assertion, as I did on CTV news recently, that we don’t have a shortage of family doctors?

Truth be told, there is an important distinction that has to made, which is key to solving the orphaned patient crisis. There are family doctors, and there are family doctors who are willing to work in a comprehensive care family practice like I do.
According to the Ontario Medical Association (OMA) website, there are over 15,000 members of the Section of General and Family Practice. These doctors have got their medical licence, are qualified to practice in Ontario, and are able to practice family medicine without any further regulatory hurdles (like getting foreign doctors licensed would entail). There are likely many more as some doctors with a family practice billing licence don’t choose a section – but let’s go with 15,000.
What’s really telling is that only about 9,300 are in what’s called a PEM (Practice Enrolment Model – where a formal agreement exists to run a family practice). The number that are in Fee For Service alone (without an agreement) but still run a practice, is likely only a couple of hundred. So at most we have 9,500 comprehensive care family doctors. The other 5,500+ do something else (hospital only work, clinical associate work, walk in, etc).

There’s a myriad of reasons why comprehensive family practice is so unappealing, but let’s look at the two main ones.
1)Decreasing net incomes over the years. It is of course, unpopular to talk about the money doctors make. The OMA has historically felt that the general public views doctors as “fat cats” and “part of the rich elite.” So they’ve shied away from talking about physicians incomes or trying to positively frame that discussion – with predictable results.
As Boris Kralj (PhD in Economics, Adjunct Asst. Prof at McMaster and former Staff at the OMA) points out, net income for family physicians has fallen drastically over the past 20 years.

2) Increasing Admin Burden. I think everybody has heard how family doctors now spend up to 19 hours a week doing administrative work, ON TOP of the time they spend seeing patients. This work is unpaid of course (there is no fee code for admin work). On a personal note, in about 2004, my office, which was already electronic, got a vpn (virtual private network). This allowed me to connect to he office from anywhere in the world. Initially, I thought it was great. I would go on vacation, spend 20 minutes a day taking care of messages and when I got back from vacation – I would not have the backlog of messages to deal with.
This past summer, I went on a hiking trip with one of my sons. He pointed out that I was now spending over two hours a day going through labs and messages. Essentially, family doctors don’t have any vacation now. I don’t care what your job is or who you are, a life without any breaks is unsustainable.

What can be done about this? How does one make family medicine more appealing? This may rub some people the wrong way but the first step is simple. Pay family physicians more. In Ontario, the most common fee billed by a family physician is about $37. (The last time I got a haircut, I paid $40). Out of that $37 the family doctor has to pay their nurse, receptionist, rent, cleaning, supplies and so on. Gets used up pretty quickly.
Additionally, you need to pay physicians for admin work. If there is 19 hours of admin work that needs to be done – it’s only fair that work is paid for. There are people who are skeptical this will work. To them I would point out that British Columbia has gotten 700 more family doctors since increasing the pay to family physicians.
You mean if you increase the income for a job, more people will apply for it? Who knew?
B.C. isn’t even the province that pays physicians the most. That’s arguably, as I have written before, Manitoba. Saskatchewans new deal is also much better than what Ontario offers.
The second aspect is to reduce the admin burden for all physicians. Many experts suggest this is a process that will take time. They are the same experts that oversaw the increase in Admin work for physicians with “oh it’s just one extra click or it’s just a simple form”.
To reduce the Admin burden significantly, one needs to drastically revamp digital health care. Get rid of eHealth Ontario and OntarioMD, and run all decisions through the Digital Health Branch of the Ministry of Health. It’s too late to unify all of our electronic medical records, but you can approve one (and only one) patient app that will allow patients to access and transfer their records to the physician of their choice to reduce duplication and waste. That’s the kind of bold steps that we need to take, not just crowing about the fact that doctors don’t have to sign hearing aid forms any more.
Look we already have 5,500 licensed family physicians in Ontario able to open up a practice. If 40 per cent did so, it would end this crisis immediately without having to resort to years long plans of modifying licensing and training requirements for foreign graduates (who in fairness are generally very good).
Do our leaders have the boldness and vision to do the right thing?
Dr. Soni Reflects on the Delays in Emergency Rooms

NB: Recently, Julia Malott spoke out on X (formerly known as Twitter) about how terrified she was about Canada’s health care crisis. She wrote how her daughter had not eaten in 18 hours as she continued to wait for surgery for appendicitis. She expressed concern about the lack of the beds and wondered if her daughter would get surgery before the appendix ruptured.
My friend Dr. Soni, who has worked in an Emergency Department for over 20 years, had, as usual, a very thoughtful and well spoken X thread of her own. (Dr. Soni was NOT involved in the care of this young woman). I thank her for allowing me to reproduce her thoughts here.
The only way these stories (about long delays in Emergency rooms) will stop being the norm, is when patients start sharing their experience like this mother did. Only voters can make federal and provincial governments change because votes are the only currency that matter. Doctors and nurses have been raising alarm bells for years without success.
Canada has one of the lowest number of hospital beds of all the OECD countries, around 2.3/1000 people. In comparison countries like Japan, Korea and Germany are around 13/1000.
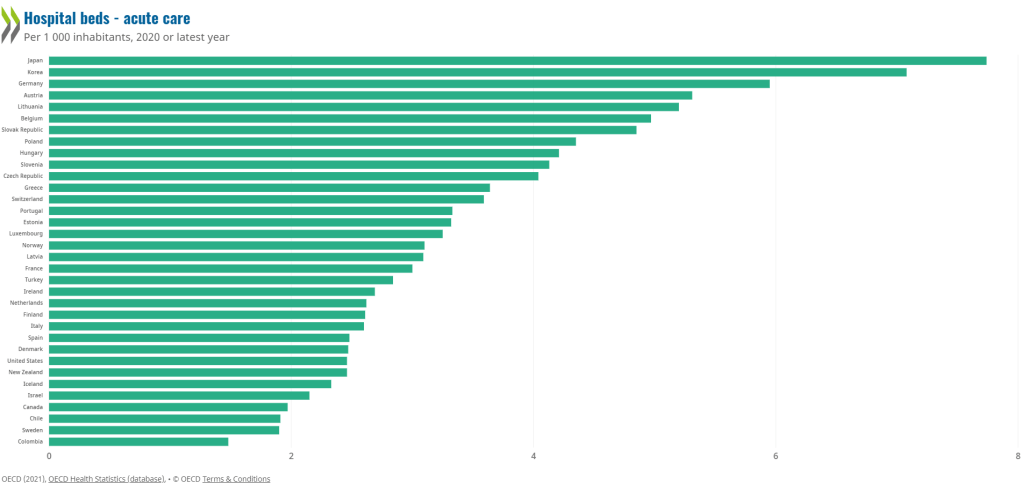
Why does this matter? Having low hospital bed numbers means that words like “flu surge“, and “winter surge” — which have been used for decades to explain away long wait times and hallway medicine, are actually not “surges.” Rather, they are the expected backlog in a system that lacks adequate beds and resources.
The population of Canada is increasing and aging. We are about to enter a silver tsunami where a large cohort of our population will be over the age of 65 and many over the age of 85. This will place unprecedented pressures on our health care system.
What happens when the hospital bed capacity is outstripped by the numbers of patients needing care? It means that the elderly patient who needs admission to a hospital bed to recover from a heart attack has no bed to go to and spends days “admitted” in the emergency department. Bureaucrats call these “unconventional spaces.” What they really are, are stretchers.

When the vast majority of the emergency department beds are being used to take care of hospital patients, that means that patients that are waiting in the emergency department waiting room, will wait for hours for care, much like this story is describing.
Media needs to scratch beyond the surface and hold government to account. Real solutions are going to require thinking beyond the four-year election cycle. What will our system look like in 20 years? How do you plan for that?
It’s going to require recognizing the backbone of our healthcare system is primary care. Family doctors are overwhelmed by administrative burden, trying to run their offices and taking care of large practises in the community without adequate resources.
Build community infrastructure with resources like palliative care so that people can remain in their homes comfortably in their last days; and sufficient homecare services so that patients can receive antibiotics and other intravenous treatments at home to ease the pressure on hospitals. These services are vastly underfunded and do not have enough staff to properly provide care for everyone that needs it in the community.
It’s going to require building more nursing homes, retirement homes, seniors services and dementia care programs, as our elderly population will be the largest it’s ever been in this country.
Incentivize and properly pay hospital nurses so that we can recruit and retain them to be able to run departments and programs properly. Currently, agency nurses make at least two times as much as a hospital nurse, and this has created instability in the workforce. Governments need to show that they value nurses and the important work that they do.
Creative solutions like interprovincial licensing of doctors and nurses and a National Pharmacare program will help. While the idea of recruiting from other countries sounds like an easy quick fix, it will not solve anything if those newly obtained doctors and nurses find themselves overworked and burning out soon after arriving to Canada. The system problems are going to impact them just as they have impacted those who are already working in the system. This type of strain is what contributes to moral distress and burn out.
The backlog in the emergency department is a reflection of multiple failing areas that create an overall system that is strained beyond capacity. With each passing year, Canada’s healthcare system has become more and more stretched, trying to provide more care to more people, with fewer resources. Throwing Band-Aids at it is like trying to mop up the floor under an overflowing sink instead of trying to figure out how to turn off the tap.
Stories like this one are happening every day in Ontario and all of Canada. Most patients and families are too busy dealing with the acute health problem to take the time to write to their MP/MPP or to go to the media. But when people take the time to bring these stories to light, a critical tipping point will eventually occur where they can no longer be ignored by government. Because votes matter.
No one who went into healthcare wants to work in a system that makes patients feel like this story illuminated. But we need more voices bringing their stories out in the open. It will improve the system for the people working in it, and for the people receiving care within it. And that is better for everyone.
What Would I Do if I Got Sick? I Would go to Turkiye.

NB. I am a consultant for Medicte, a medical tourism firm that connects people with the Acibadem Health Group in Turkiye. I appreciate my two loyal fans may read this to be an “advertorial” – but it does represent how I feel.

Recently, Leger released the findings of a survey that polled Canadians on their thoughts about the health care system. 70% of Canadians worried about not being able to get high quality health care. Surprisingly, only 37% thought the health care system was poor – did 63% not need medical care recently? But the number that should demoralize all of us is that only 17% feel the system will improve.
Like everyone else of a certain age, I’m coming to the realization that the one fight I won’t win, is the battle against time. More of my friends and colleagues are developing health issues. While I’m blessed to be in good health, like 83% of Canadians, I realize that the current health care system (which doctors call horrific and inhumane ), will not provide the access and care we should expect as standard in this country. I can only see things getting worse in the near future.
It does not help that I live in the health system every day. I’ve watched patients I really care about suffer in ways that I would not have imagined possible. Young people with cancer not getting treatment for three months. People with joint pain waiting a year for surgery. Patients developing complication after complication while on wait lists to access necessary treatments.
Most heartbreakingly, I see the toll that the burnout of working in such a hellishly damnable health care system is taking on doctors, nurses and other allied health care professionals on a daily basis.
That’s why I recently made the decision that if I, or someone in my family needed health care, I would seek care outside of Canada. I am not alone in this. The data is hard to get at, but going back as far as 2014, between 52,000 to 217,000 Canadians were seeking health care outside of Canada annually.
There are a variety of reasons to seek care outside of Canada, and specifically Türkiye:
- Getting immediate care. I could get hip surgery next week, not next year. Cancer patients get all the tests they need done within a week, not three months like I’ve seen.
- Getting treatments that are not available in Canada. Canada offers a host of great medical treatments, but many are not covered by government plans. Lap Band surgery is one. New, emerging radiation therapies for pancreatic cancer is another. There are more. All of these are available in Türkiye.
- Getting better allied health care support. Canada has GREAT nurses and other allied health care workers. But the system does not let them care for patients the best. Last time I was on call at my hospital, I overheard the nurses talking about how they each had 7 patients to look after for the shift. The safe number for an acute care hospital ward is 5 patients per nurse. We have excellent nurses but if you are constantly working at 40% over capacity, things are not going to go well. At the Acibadem hospitals in Türkiye, they have 4 nurses for 15 patients (3.75 patients per nurse).
- More cost effective care. I’m fortunate I can afford to pay out of pocket for care if needed. Worst comes to worst I’ll put off retirement for a couple of years to pay for things if necessary. But even I would have trouble with $200,000 (U.S.!) that B. C. resident Allison Ducluzeau spent on her cancer care. Costs in Türkiye for most procedures I looked at are generally less than half of what it costs in the U.S.
- First World Standards for Health Care Treatments. All of the Acibadem hospitals are JCI Accredited (the global leader in health care accreditation agencies). This puts them on par (and in some cases better) than top European hospitals.
- Türkiye is a well sought after Medical Tourism destination. Medical Travel Market recently highlighted 12 reasons why Türkiye was so well sought after including cost, world class facilities and cutting edge treatments. 1.2 million people went to Türkiye for medical tourism in 2022, mostly from Europe.
As part of my consulting work, I went on a fact finding tour to Türkiye and visited the Acibadem hospitals. To say my jaw dropped would be an understatement.

The hospitals (there are 21 in the Acibadem group) look like hotels. Each room is private. The wards are immaculate. All of the staff were incredibly attentive (and yes, spoke English).




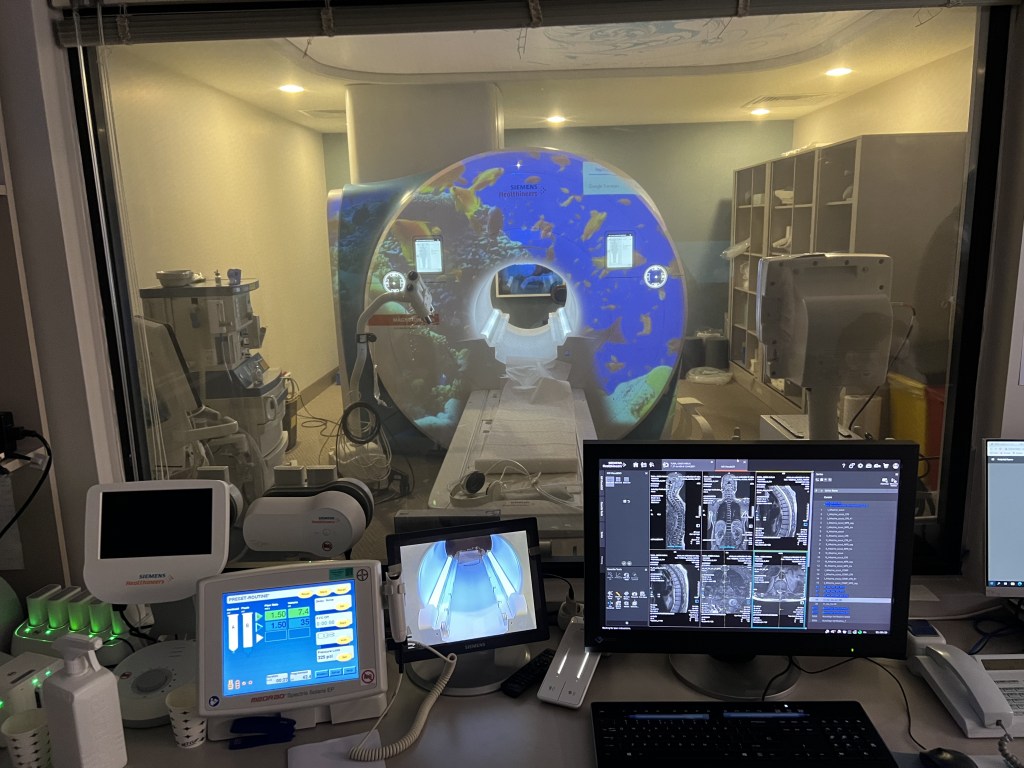
I asked to see the MRI, and the staff wanted to know which one (!). Their approximately 170 bed hospital had THREE MRIs, specialized for different conditions. This is on top of the CT scans, gamma knives (cancer treatment), PET scans etc etc. All of the equipment was brand new. I especially liked the MRI that projected a movie onto the equipment, to help children stay calm during the procedure.



I also ran into a couple of top ranked Turkish footballers (soccer players) while there. The Turks are as crazy about football as we are about hockey. Their top athletes go to the Acibadem group.
But what’s more impressive than the top ranked doctors, nurses and equipment is their philosophy of how to provide health care. If you were to sadly, get cancer, you would see all the specialists you need to see (surgeon, medical oncologist, radiation oncologists etc) on the same day. Any tests you need would be organized sequentially and rapidly over the next couple of days (if not the same day). You would have a full treatment plan within a few days.
Contrast this with Canada where you have to have an appointment with one doctor, then wait x number of weeks to see another then x to see another like my patients currently do. All while the cancer continues to grow.
Also, for the record, I did wind up getting care myself at Acibadem. Bad teeth run in my family, and so I went for a dental check up. The dentist examined me, put in two fillings, got the oral surgeon to come by and took out two teeth that were beyond hope, all during the same visit. This would have taken multiple visits in Canada. You could say I put my money where my mouth is. And yes, the care was excellent.
I appreciate this sounds like an advertorial. But the reality is that more and more Canadians are getting frustrated with the long waits for health care and seeking care outside of Canada. It may have started off with people seeking lower cost cosmetic surgery, but now things like orthopaedic surgery, cancer treatments, organ transplants, dental implants and even cutting edge infertility treatments can be had for those willing to travel.
There is never a guarantee of a successful result with medical treatments anywhere (including Canada). If considering leaving the country for care, people should do their due diligence. Make sure you deal with a reputable firm and first rate hospital.
I’ve made my decision, and I know where I’ll go.
If you or anyone else would like to explore options for out of country health care, contact Medicte for a free consultation.
OMA Needs to Communicate Better About Status of Negotiations
Negotiations between the Ontario Medical Association (OMA) and the Ministry of Health (MOH) on a new Physicians Services Agreement (PSA) began this past fall. The first set of bilateral meetings were in mid-October. This years negotiations present a particularly complex challenge as not only is the OMA trying to negotiate a new four year agreement for physicians, but it also has to determine how much of an increase physicians will get this year (more on that later).
Given that we are a few months into the process – I think the OMA as an organization is really not doing a very good job of communicating the status of the Negotiations with its members. The OMA really needs to increase some of the transparency around the negotiations process.
In fairness, there are somethings about negotiations that simply can’t be divulged (and I fully support this and members do need to accept this):
- The mandate for negotiations must be confidential, to prevent the other side from knowing what our bare minimum acceptable increase is
- The detailed discussions between the Negotiations Task Force (NTF) and the MOH must also be confidential (a lot of stuff that goes back and forth is hypothetical – and to protect the integrity of the process – you can’t disclose this to 40,000 + people)
- The briefings presented to the Board and the Section Chairs must stay confidential as well (for the same reasons above).
- NB – If we wind up in arbitration, the asks at arbitration are public.
So what should the OMA be informing members about then, given what’s usually a “cone of silence” around negotiations? Well, put simply, there are a number of things that are part of the negotiations process, outlined in public documents readily available to all members. The OMA needs to recognize some members (not just me) will read and wonder about these. (Although I’m probably one of the few loudmouths who’ll publicly write about it).

For example, the Binding Arbitration Framework, under which negotiations are now held, is posted on the OMA website for all physicians to see. The framework is pretty clear. After 60 days of negotiations, either side can ask for mediation. They don’t have to, but they can.
We are over 60 days. Perhaps mediation is not needed yet (which would be a good thing). But the OMA can, without compromising the negotiations tell members something like “while we have been negotiating for x number of days, at this time the process continues and we neither side has called for mediation.” It would at least let members who follow this closely know what the stages are.
Similarly, it would be quite reasonable for the OMA to list the dates of the meetings with he MOH and a general list of what they are talking about. Eg Oct 19 met with MOH to discuss Primary Care models, Oct 21 to discuss backlog in radiology etc. (I have no idea when the meetings with the MOH were or what they talked about btw – I’m just pointing out what could be said).
Finally, there appears to be radio silence about the part of the last contract that directly affects this year. This contract was completed and ratified by members and is public knowledge. The parts of concern are:
21. ….the parties will establish a committee that will meet on a quarterly basis…..to review the expenditure calculations. Through this committee, the parties will agree to a best estimate of the year 3 (2023- 2024) PSB expenditures in accordance with paragraph 6 by December 15, 2023.
22. Any agreements reached by the Government with respect to any new physician payment program or addition to an existing program which was not the subject of a proposal by the OMA during the negotiations leading to the agreement for the 2021-2024 PSA will not be included in calculating the total PSB expenditure …..”
It’s obviously past December 15, 2023. Which means we should have an agreement on the PSB expenditures by know. This information is critical to determining how much of an increase we get this year. The OMA had told us that:
“Conservative OMA projections indicate an expected Year 3 increase of 2.8 per cent, with a range of 2.1 per cent to 3.6 per cent”
But if the expenditures are too high, then we potentially get a zero percent increase. My friend Paul Hacker did an EXCELLENT job of explaining this here:
As an aside, some of you wondered why I endorsed him for OMA Board Director. It’s because of stuff like the above link. He knows the Board needs to provide proper oversight on the process and ensure it’s explained to members.
Anyway, perhaps this date got pushed back. This wouldn’t surprise me. The MOH Negotiations team was never able to get data on time in the past (there was always an excuse, except for the truth – that they are generally incompetent).
But the OMA should simply tell members this. Remember last year when it was announced to primary care docs that the repurposing of the preventative care bonuses couldn’t be mutually agreed on, and so was delayed for a year? Do the same thing and say the deadline couldn’t be met and you continue to work on it. But don’t just ignore the deadline and hope no one will notice.
Communicating better would also be beneficial for the NTF. There is no task force at the OMA that is more controversial, and gets more….attention…from members than the NTF. Yet what’s missed is that the NTF works really really hard. I remember some of the 18 hour days they put in when I was in various roles at the OMA.
But when communication about the process, and the work they are doing is substandard, members won’t appreciate all that. They’ll simply blame the NTF for what goes wrong (e.g. if we were to get zero percent this year). It would be foolish in the extreme to suggest everyone will love the NTF if they just communicated better. But better communication would at least blunt some of the criticism that will come their way.
Hopefully, the OMA as an organization will recognize this.
Will Medical Political History Repeat Itself in 2024?

“The Wheel of Time turns, and Ages come and pass, leaving memories that become legend. Legend fades to myth, and even myth is long forgotten when the Age that gave it birth comes again.”
—The Eye of the World, Book I of the Wheel of Time Series of Novels.
One of the advantages (?) of being old, is that you can see when history is about to repeat itself. Having followed medical politics for over three decades now (!), I continue to be amazed at how things keep circling, just like in the Wheel of Time series of novels. Unlike those books however, the Wheel in Medical Politics (WIMP?!?) would seem to come around every decade.
Case in point is the current crisis in family practice. I won’t bore with you the details yet again since this issue is all over the news. But I will bore you by pointing out that this is currently the third major health care crisis in my career.
In the late 1990s, there was a significant shortage of family physicians (sound familiar?). The shortage was made worse by poor payment for family physicians and poor working conditions. The Ontario Medical Association (OMA), which was supposed to represent all physicians, was widely viewed by the members at the time to be sorely lacking in helping family physicians. This led a few physicians (among them Drs. Sharla Lichtma/Rochelle Schwarts/Suzanne Strasberg) to form the Coalition of Family Physicians (COFP).

Being politically savvy, they went out to the media and said things that the OMA, for whatever reason, did not. Not only did they get the attention of the press, they were (regardless of whatever revisionist history may suggest) instrumental in forcing the government of the day to institute Primary Care Reform and bring in the capitation models of funding for family practice.
Their leaders also ran for OMA positions, with one of them, Dr. Suzanne Strasburg, eventually becoming the OMA president. It would be erroneous of me to suggest the OMA suddenly became an organization that had the undying love of its members, but the reality was that there was a noticeable shift in tone of their messaging when various members of the COFP got elected to the OMA Board.
Fast forward to the mid 2010s, and, once again there was a (you guessed it) crisis in medicine. This time, the crisis was created by militant Health Minister Hoskins, who was hell bent on doing things his own way. It’s not without reason that one grumpy old coot coined the moniker “Unilateral Eric” for him.
Hoskins and his belligerent deputy Minister Bob Bell were so certain that what they were doing is right that they never bothered listening to the many intelligent people who tried to help them. Shockingly for most of us, instead of defending doctors, the OMA got into bed with Hoskins and Bell (aack! now I can’t get that image out of my head) and actually agreed on a tentative contract that stabbed doctors in the back.
Once again, when the OMA couldn’t deliver for physicians, a breakaway group of doctors got organized on Social Media. They were led by a strong crew of doctors that included the likes of Drs. Nadia Alam, Paul Hacker, Silvy Mathew and advised by people like Dr. Paul Conte and too many others to named. Despite being weighed down by an ancient, crotchety bugger they went and said and did things that the OMA couldn’t. They caught the eye of the media and the hope of the membership. Eventually, some of them (you guessed it) wound up on the OMA Board.
Once again, while the OMA hardly became beloved by members, there was a noticeable shift in the tone from the OMA. Remember the ”Not a second longer” ads?


And yes, Dr. Alam (and the guy who came in on her coat tails) both eventually wound up being President of the OMA.
As we head into the mid-2020s (!), the Wheel of Time is turning, and the Age is now being reborn. Once again the crisis in Family Medicine is in the forefront. Once again, the OMA is seen by many to be lacking in defending the profession.
N.B. I really do appreciate the work of most of the staff at the OMA but the reality is that the OMA has spent much of the past couple of years pushing their “Prescription for Ontario.“ To be fair, it’s a very good document with many positive ideas for change. But the blunt reality is that no one in government asked for it, any similarity to what government is doing is purely co-incidental and not because they are listening to the OMA, and the unrelenting focus on it makes members feel as if you the organization is not advocating for their own personal well being.
And of course, we now have the Ontario Union of Family Physicians. A breakaway group that has gone out and said and done things the OMA can’t. Led by Drs. Ramsey Hijazi, Britt Harrison, Vakar Khan, Alex Duong and too man others to name, the group has, in very short order:
- set up an incredibly slick and well functioning website
- been active in the media talking about why family physicians are quitting and not being afraid to mention that poor pay is (along with the admin burden) a root cause.
- Began a job action campaign that the OMA can’t
- and yes, one of their own, Dr. Ramsey Hijazi, is now running for OMA Board (along with Drs. Paul Conte and Paul Hacker). Full disclosure – I’m voting for all three of them, and you should too – and no, they didn’t know I would endorse them in this blog.

It’s easy to get cynical about medical politics when one sees how things keep circling. Truth be told, I’ve had my own moments of pessimism where I’ve wondered why things don’t change permanently. But the reality is that any big organization will have a tendency towards inertia. That’s just life.
But what’s also reality is that these organizations also significantly benefit from having people who are widely viewed as outsiders, or “disruptors” come in and shake things up. This is a healthy thing (whether the organizations thinks so or not). And it seems, in 2024, we may get that again.
Supporting Education the Key to Helping Developing Countries
I recently had the honour of being a guest speaker (along with the amazing Dr. Nadia Alam) at a fund raising dinner for Friends of Namal, an organization that provides university scholarships for students in Pakistan. The following is an abridged version of my speech.
I want to tell the story of a man who was born in Surat, in the State of Gujarat in India in 1933. He moved to Karachi in 1947 during the Partition, and as a teenager witnessed many of the horrors that occurred during that time. He was academically bright, but his family was poor and there was no way that he could afford a University education. However, in 1951 he became aware of a foreign students scholarship from McGill University, applied, and was successful. Four years later he became the first student in the history of McGill to complete his Chartered Accountant and Registered Industrial Accountant degrees simultaneously.

After that, he went back to Pakistan and worked for a number of years to support his extended family (his parents had died when he was young so he took care of his sisters who had raised him). In 1966, he and his young wife had a baby boy at the Holy Family Hospital in Karachi. Two years later, he went to Africa with his family as there was a better opportunity there. In 1972, when things got bad in Africa, he decided to move to Canada with his wife and son.
The rest of his family thought he was crazy. ”Where is this Canada place?” ”How far away is it anyway?” “Are there even any muslims there?”
And indeed, there was not much of a Muslim community in Toronto at the time. There was the Jami Mosque, one Halal meat shop on Gerrard street, and, well, that was about it. Not like today when, by the blessing of Allah there are mosques and halal restaurants seemingly every few blocks.
As you may have guessed by now, that man was my father. Because he brought me here at a young age, I didn’t really appreciate the significance of such a move. Truth be told, I really didn’t have great study habits. But one day, when I was visiting my Nana Abba (maternal grandfather), he recited a Hadith (a saying of the Prophet Muhammad, PBUH):
“The ink of the scholar is worth more than the blood of a martyr.”
I am aware that some scholars feel the Hadith is weak, but the sentiment is a good one and fits with Islamic principles. I took that message to heart, began studying harder, and was fortunate to have graduated from the University of Toronto Medical School in 1990. My Nana Abba came to my graduation ceremony. After that, he told me clearly that I was blessed to be an educated man, but now I had a responsibility to help others who wanted an education. I had to pay back my blessings by helping other people, no matter from what walk of life they came from.
So, after I finished my residency, I took over a family practice in a small town called Stayner……and my parents thought I was crazy. ”Where is this Stayner place?” “How far away is it anyway?” “Are there even any muslims there?” Funny how that works.
But I have now been there for 31 years, taught many medical students through the excellent Rural Ontario Medical Program, and seen the community grow significantly. Where once the muslim population of the area doubled just by me getting married, there are now 50 or 60 families, three halal restaurants and a Musallah (prayer site – not quite a mosque).
Along the way, I managed to run into Dr. Nadia Alam through some medical politics. She convinced me that I should run for OMA Leadership (I still haven’t forgiven her for that by the way). Eventually this lead to me being the President of the Ontario Medical Association (I was the second Pakistani born president in its history, Dr. Alam was the first). This gave me the opportunity to meet many health care leaders, and politicians, and achieve things I never thought possible.

When I look back on this, I ask myself “How did this happen?” To my mind, there are two reasons. First and foremost it is because it is a blessing from Allah. Nothing happens without His will and whatever I have achieved is a result of His kindness.
The second reason of course, is because somebody gave a deserving young Pakistani student a scholarship in 1951, to let him get an education that he otherwise could not have afforded. This then, is the power of education and this then is why it is incumbent upon every muslim to get an education. Another Hadith:
“Seeking knowledge is an obligation upon every Muslim.”
Note the wording. It’s not a request. It’s not a suggestion. It’s an obligation, a command if you will, that every Muslim MUST seek an education. Every Muslim. The Prophet PBUH did not believe there were “types of muslims” and did not distinguish between gender for eductation. Therefore, it’s also an obligation for those of us who can, to HELP other muslims get an education.
We’ve seen what can happen when just one deserving student gets an education he could not otherwise have afforded. Imagine what can happen if five students do. Or ten. One hundred. More. Education is the key to making a better society and a better future for any country. I encourage those of you who are able to visit the Friends of Namal website, and contribute generously.


DFCM at Temerty Faculty of Medicine’s Stunt is DANGEROUS for Physicians AND Patients
I’ve been involved in medical politics for some time and in health care for much longer. I’ve seen a lot of foolish things. And yet, I confess, I’m still dumbfounded when some really smart people come up with a really stupid ideas. I guess I’m just a slow learner.
The most recent of these ideas comes from the Department of Family and Community Medicine (DFCM) at Temerty Faculty of Medicine. (Temerty is the name for the University of Toronto Medical School – and no, I have no idea when or why they changed their name to Temerty). In an attempt to address the crisis in Family Medicine, Drs. Pinto/Kiran and Martin would like the governments to declare a state of emergency in access to primary care.
Do I understand wanting to draw more attention to the crisis in Family Medicine? Of course I do. Family Doctors are planning to leave the field in droves. Compensation for family medicine has failed to keep up with inflation much less given them a raise. The admin burden makes one feel like Sisyphus (In Greek mythology Sisyphus was dammed by the gods to roll a boulder to the top of a hill only to have it roll suddenly back down to the bottom when it got close to the top and thus be forced to roll it up again. A more apt description of the family medicine paperwork burden I have never seen).
Heck across the country our whole health care system is in crisis, not just family medicine. Patients are not getting timely specialist care (some even choosing euthanasia as a result) as well as family practice care, resulting in worsening health care outcomes for all Canadians. We should be screaming about this.
But I honestly don’t think Drs. Pinto/Kiran/Martin (who combined have more letters after their name than the entire alphabet) could possibly have thought this recommendation through. Frankly, I’m genuinely left wondering if they even know what the government declaring “a state of emergency” means. The only way to enact this, is to invoke the Canada Emergency Act.
This Act clearly lays out what governments can do to solve a crisis in any particular area. And it’s not pretty. It includes:
- giving the government the “ability to make orders or regulations that are believed, on reasonable grounds, to be necessary…”
- Directing specified persons to render essential services…
- Regulating the use of specified property, including goods…
- The imposition of fines or imprisonment for contravening on any of the measures declared..
In short, having the government declare a state of emergency gives them a whole lotta power to do a whole lotta things. I guarantee you not all of those things will be smart.
No one in their right minds is going to argue with the issues identified in the letter three doctors wrote about:

The crisis in family medicine is real. There has been a lack of investment in primary care. This will get worse. This will cost the health system more money in the future if we fail to fix the problem. And yes, thank goodness somebody other than a cranky cynical old country doctor wants a significant overhaul and feels that “modest changes are not enough”.
But – to tell the government to enact a state of emergency, giving the same bureaucrats who have completely screwed up the health care system for the past thirty years almost unfettered power is not the solution. Let’s look at some of the goals of these three doctors:

If there is a state of emergency – do you know how these pointed headed bureaucrats will take “decisive action” to “ensure every person in their jurisdiction has equitable access”? You think they will licence more physicians? You think they will allow Ontario Health Teams (OHTs) to have strong physician leadership (which is the ONLY thing that has been proven to work in accountable care type organizations like these OHTs)?
I got news for you. The pointy headed bureaucrats will simply mandate zones, unilaterally determine how many patients a doctor must roster, and will make decisions in the interests of “urgency” given the new powers they just got from a state of emergency to show they are doing something.
Say for example the recent situation when Royal Victoria Hospital had to close down their obstetrics service. Hell that Gandhi fellow delivered babies 20 years ago, he probably hasn’t forgotten what to do – send him there to cover so it doesn’t close, he’s only 45 minutes away. Or a hospital about close their ER again – force a local doc who hasn’t worked in ER for 15 years to do so. 7,000 patients without a doctor in a certain town? Have each family doctor take a couple hundred more – even though those docs are already working night and day. (Trust me – these ideas will not sound outlandish to bureaucrats.)
Drs. Pinto/Kiran/Martin know that to make inroads into solving the primary care crisis you need to do three things:
- increase the payment to family physicians to reflect the work they do. Decades of sub inflationary wage increases (cuts by another name) have made it untenable to run a family physicians office. Pay family docs more and don’t be afraid to say so.
- The OHTs actually have potential for improving health care, but they need strong family physician leadership – not any other health care professional (and certainly not bureaucrats) – family physicians need to lead this. (The OMA has plenty of evidence on this and has shared with the government and will share with you).
- Interchangeable IT technology that allows easy access to patient data and thus minimizes the admin burden.
The only reason I can think of for doing this is some sort of political stunt to embarrass the politicians. Heck I agree politicians should be embarrassed for how badly they’ve messed things up. But to do it in a way that gives them more power (not less) instead of demanding a true collaboration with family physicians doesn’t strike me as a very smart move at all.
