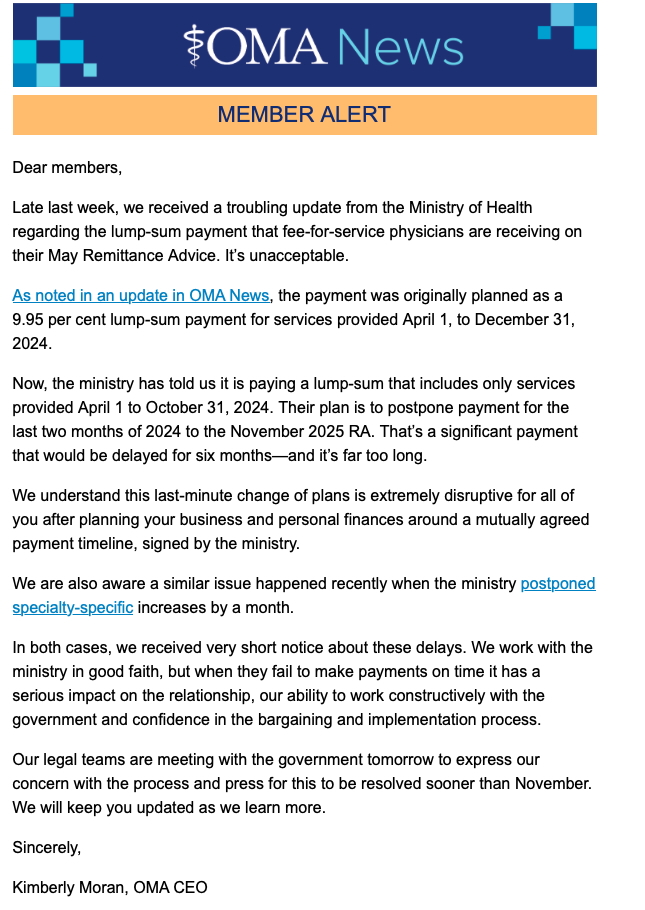
Last Friday (May 2), in what was a classic Friday afternoon bureaucratic dump, the OHIP bureaucrats at the Ministry of Health announced that they wouldn’t be paying the full amount of back pay owed Ontario’s doctors, as per the arbitration award. This was a unilateral decision on their part. It was contrary to what was in a signed agreement, and the OMA Board was notified at the last minute. (OMA CEO Kim Moran’s email is attached to the bottom of this blog). The bureaucrats promptly ran away an hid for the weekend hoping this issue would go away (kind of like how Sam Bennett cowardly hid from the press after putting an elbow to Leafs goalie Anthony Stolarz head).
This is, in my opinion, the latest attack on physicians as a whole from Ministry of Health (MOH) bureaucrats, who clearly are more interested in trench warfare than working co-operatively with Ontario’s doctors to improve health care for the citizens of Ontario. Don’t believe me? Consider the following:
The bureaucrats had the option of realizing that provinces like Manitoba/BC/Saskatchewan and even Alberta(!) recognized the need to work with their doctors and come up with a funding formula for them. Instead they chose to drag Ontario’s physicians through a protracted (going on three years now) and highly antagonistic arbitration/negotiations process.
Not only that, in response to now multiple stories of people lining up to find a family doctor in the press, their response was that there was “no concern” about the shortage of comprehensive family care physicians. (Seriously, how out of touch must they be to think that that type of Orwellian double speak is going to work in Canada).

Frankly, this inept, combative and dismissive treatment of physicians is just par for the course for this bunch of bureaucrats. It saddens me, but it doesn’t surprise me.
No blame for this decision should fall to the OMA. They did negotiate a signed agreement (as per Ms. Moran’s email) and they clearly were not notified about the unilateral change until far too late. So the unilateral action is not their fault.
But….
What the OMA can, and should be held accountable for is how they proceed from here.
I don’t want to seem overly difficult here. If I truly was an obstinate person, I’d try to get a job at the Ministry of Health – perhaps on their Negotiations Team. The reality is that I actually have a long history of working co-operatively with government to improve health care in my neck of the woods.
I’m serious. In 2001 I helped bring in the first stage of Primary Care Reform called the Family Health Group. In 2004 I was one of the lead physicians who brought in a capitation model of payment for family physicians (it was initially a Family Health Network and it eventually evolved into a Family Health Organization). From 2007 -2013 I was the founding Chair of the Georgian Bay Family Health Team and From 2013-2015 I was the Health Links lead physician in my area.
And in each of these roles I worked closely and co-operatively with government to try to improve the health care needs of the patients in my area.
But – in those days, the bureaucrats wanted to work with doctors. They wanted to co-operate to improve health care and they were genuinely concerned about the lack of family physicians providing comprehensive care. They didn’t want to play power games with physicians or harass them or do dumb things like the current crop just did.
It’s important for the OMA to (finally) realize that there really is no hope that they can work with the current lot. They’ve already dragged us through three miserable years of negotiation/arbitration and fought us (thankfully often times stupidly – as even the Arbitrator pointed out) – for the sake of…….. I don’t know why really. Maybe it’s a power play? Maybe there are just bullies?
Recognizing the obstinance of the MOH bureaucrats is why I was proud (and still am) to have my name on an Op-Ed in the Toronto Star last year advising Family Medicine Residents to NOT start a practice in Ontario at this time. But I have to tell you the blowback from the OMA was saddening to me. I will not mention names – but one senior exec told me that the OMA was working well with the Government. Worse, one senior physician leader texted me the following:

Remember – at the time this text was sent to me – we had already been locking horns at the negotiations table for two years and the government had done absolutely nothing to solve the family medicine crisis. Perhaps the physician leader felt the relationship was “best ever” because at least they weren’t sabotaging doctors left right and centre like the abhorrent Eric Hoskins did.
Despite all of that, there was some movement forward with arbitration. While no where near what other provinces got, it at least recognized the need to fund health care better, and provided hope for funding for offices, clinics, and frankly other badly needed resources.
Now the MOH has decided unilaterally to not pay, or pay whenever they feel like it, so we are back to – do NOT start to work in Ontario.
At any rate – as mentioned, while the OMA cannot be judged on decisions by the Ministry, what the organization does next will be telling. Will they finally recognize that the current lot of bureaucrats simply cannot be dealt with by reason? Will they recognize that physicians are essentially being bullied by these ruffians and the best way to deal with a bully is to stand up to them? Will they take legal action (according to Ms. Moran’s email – there was a signed agreement which the MoH is now in violation of)?
I don’t know the answer to any of the above. But I can only hope that the current Board recognizes that there is no hope of working in good faith with this lot of bureaucrats and that strong, frankly militant actions, are needed to support the members.
Addendum: After I published my original blog, an anonymous colleague asked that I publish a link to a survey about this issue. I’ve therefore appended my blog and ask all Ontario physicians to click on the link below and honestly reply to the questions:
https://www.surveymonkey.com/r/W2ZPMCC