I’m honoured to have Dr. Silvy Mathew guest blog for me today. She’s a former member of the OMA Board, former member of the Physicians Services Committee, has a Master’s in Health Policy and Economics, a Certificate in Global Health and is hands down one of the smartest people I know.
Health care in Canada is governed by the Canada Health Act, a federal act that essentially states that medically necessary care provided by physicians and hospitals, will be covered by public insurance and administered by each province.
The Act was passed in 1984, and is reflective of the type of acute medical care practiced at the time. However, in 2023 (and for at least a decade prior), medical care, through technology, medical advancements and aging, has changed drastically. Publicly covered care now, however well intentioned, is sorely lacking. Ironically, because of that, it is also very expensive.
For exampe, we lack public pharmacare for adults despite being promised this by 2006 by then Prime Minister Paul Martin. (There is some pharmacare for seniors and children).
We lack dental care. We lack appropriate home care in an aging population that is getting weaker and frailer. We lack coverage on physiotherapy. In an era of increasing mental health burdens we lack psychotherapy.
The list goes on and on, notwithstanding the severe social issues that contribute to many of these issues (healthy food, exercise, housing and all the other social determinants of health).
Because we have not invested upfront, we pay significant costs in expensive procedures, prolonged hospital stays, and medications much of which could be minimized or avoided.
Why does it matter?
McKinsey Global Institute published a prospective analysis of 200 countries, looking forward on the impact of 52 diseases over the next two decades to quantify the social and economic gains if health is made a priority by government and private sector. They quantified the value of health to the economy and showed that if using the existing interventions we have today, we can reduce disease burden by 40% in the next 20 years and extend “active middle age by 10 years”. This translates to an economic return of $2-$4 for each $1 invested. That’s remarkable.

What’s the hold up? The lack of foresight, upfront cost and political inertia is costing us.
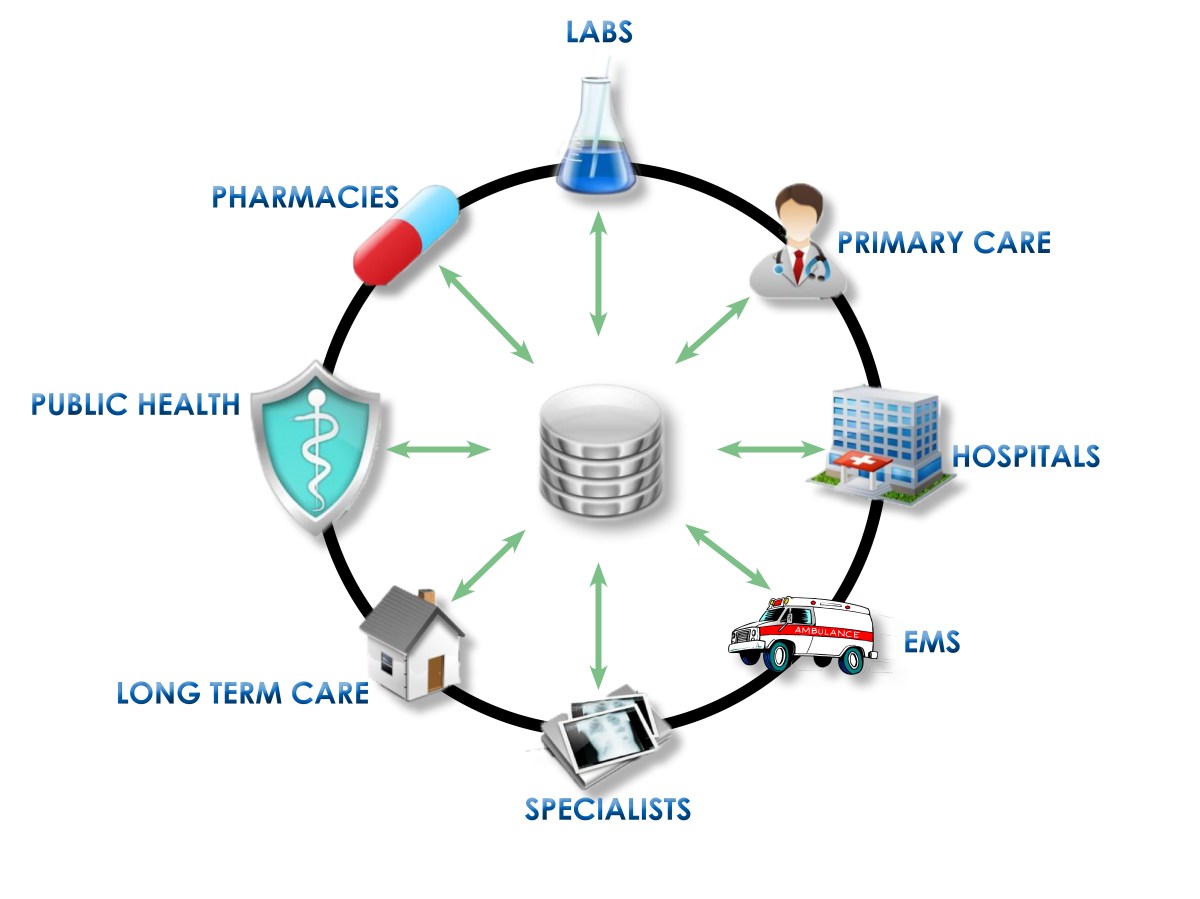
We have a shortage of healthcare professionals, and we use the ones we have, in extremely inefficient ways. For example, the lack of a proper digital health infrastructure in Ontario (like they have in Turkiye!) results in duplication of services, poor coordination, and inconsistent delivery of health care. Even the electronic services we DO have don’t capitalize on Artificial Intelligence (AI).
Technology advancement is a double edged sword. There are benefits to patients in terms of ongoing updated guidelines for care. But health care workers are having to do more, monitor more and change practice styles more, all leading to more individual HCW time.
Each test, often results in further testing or reassessment down the line, which compounds the problem. It’s rare that physicians just close the door on one issue a day.
Again, at the time of the Canada Health Act, we were practicing acute, limited health care. Today’s world is focused on prevention and chronic illness with monitoring. That shift has placed a huge burden on physicians time to review, inform/educate, coordinate new referrals and remind individuals to do monitoring. Much of the time, it seems like we still don’t know how much benefit we will get from this. Hopefully the data will show we were correct to do this.
To collect and review the data though, we would need better digital systems to capture the information, which we don’t have.
Some people imply this will be managed with more “healthcare team members”. I think a huge solution for this particular issue is investing in technology and AI solutions.
Right now, we are trying and failing at holding back an avalanche. We have technological advancements, but limited access to those. We have lack of integration of our digital infrastructure. An ageing population is leading to increased needs. But an aging health care work force is seeing retirements and illness leading to less access. New providers are available but their impact is less clear due to lesser training and duplication of services leading to increased costs. Delayed diagnoses are leading to worsened health outcomes and more expensive care. There is less preventative care due to a shortage of family physicians which leads to delayed diagnoses, worsened health outcomes and more expensive care. Lack of care giver support and home care support means that people are leaving the workforce to care for ill relatives which leads to hospital dumping. Burnout is endemic in health care, due to a feeling of disrespect and an inability to practice best patient care.

And so, physicians are in all areas of the country are giving up and closing their practices.
In the meantime, while we wait for our wishes to come true, there is opportunity to push the envelope and to drive change. People are desperate and they want options.
When access to health care is inadequate, people will choose out of jurisdiction options for delayed procedures and even screening tests. There is a moral hazard involved. People are taking risks by going elsewhere under the assumption that they will be taken care of properly.
However, with any challenges, there are opportunities. Some “non-medically necessary” medical tests (eg. screening for vitamin D) are not covered by medicare. However, it’s increasingly viewed as an early intervention. We will only see technology increase these options as better screening methods become available, and governments delay paying for them. Perhaps instead of waiting for open heart surgery or stenting, there may come a day where preventative procedures can be used to dissolve plaque in the heart arteries.
Health care faces inescapable and exponential change. However, it is unlikely, at least in the near future, that Canada (or any country’s) public health system will be able to keep up with technology and demand.
Oh for some strong, principled leadership that can see these challenges and address them head on, without resorting to political sound bites.
•